China’s Health Diplomacy during Covid‑19
The Belt and Road Initiative (BRI) in Action
SWP Comment 2021/C 09, 26.01.2021, 8 Pagesdoi:10.18449/2021C09
Research AreasInternational cooperation in the health sector has been a firm component of China’s Belt and Road Initiative (BRI) for over five years. Since the outbreak of the Covid-19 pandemic, the Chinese leadership has been promoting this aspect of the initiative (“health silk road”) as essential to building a “global community of common destiny”. The pandemic has revealed the strengths of the BRI and the way it functions. China’s health diplomacy is farsighted and strategic. Beijing has been linking measures to combat the Covid-19 pandemic in aid recipient countries with the prospect of post-pandemic cooperation within the BRI framework. Above all, Beijing wants to be perceived internationally as a “responsible great power”.
The West’s often narrow focus on the qualitative defects of Chinese aid fails to recognise that, in the absence of traditional aid donors, Beijing has supported many third countries effectively and extensively. To counter China’s increasing influence in regions that are strategically important for Germany and Europe, greater sensitivity is needed to the geopolitical implications of the pandemic, as well as specific European proposals for third countries for the post-pandemic period. In parallel with more commitment at the multilateral level (for instance within the World Health Organisation, WHO), other options include strengthening bilateral initiatives (e.g. via regional EU+x formats) and coordination with the new US government under Joe Biden.
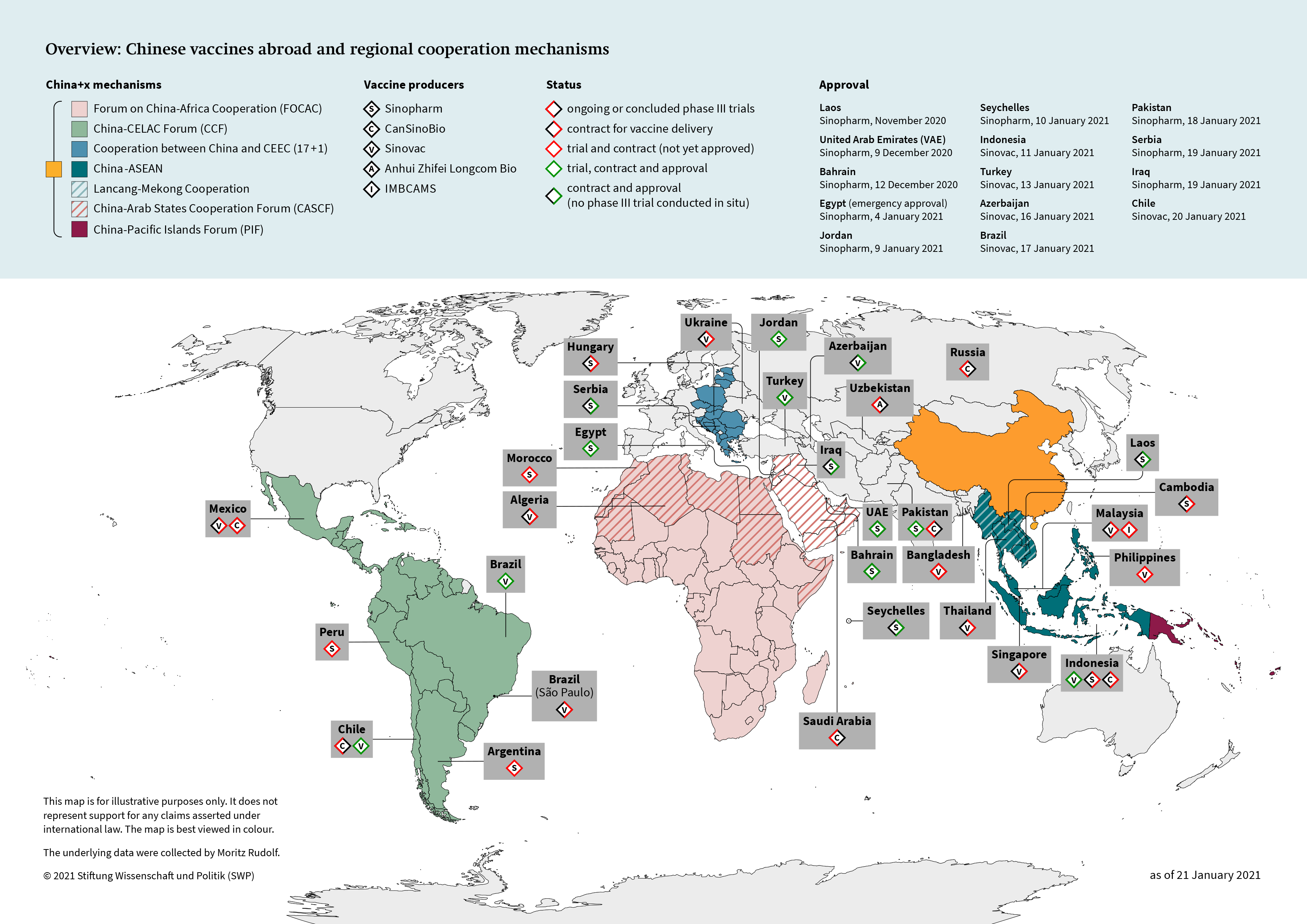
On 9 and 12 December 2020 the United Arab Emirates (UAE) and Bahrain were the first countries to approve a Chinese coronavirus vaccine. Other countries, especially in the Global South, have announced that they intend to do likewise soon (by 18 January 2021, Egypt, Indonesia, Turkey and Brazil, among others, had approved Chinese vaccines). It is realistic to assume that China will play an important role in vaccinating the world’s population. This would be consistent with the narrative promoted by the Chinese leadership: China is a responsible great power. Since the outbreak of the pandemic, China has linked its contribution in combating the virus to President Xi Jinping’s foreign-policy prestige project, the Belt and Road Initiative (BRI).
Health as Part of the BRI
Health has been on the BRI agenda for over five years. In March 2015 the framework document Vision and Actions on Jointly Building Silk Road Economic Belt And 21st-Century Maritime Silk Road already listed cooperation to prevent and contain epidemics among its objectives. According to official BRI documents, health cooperation also includes:
-
training programmes for medical staff;
-
capacity-building for public health crises;
-
emergency medical relief for crises;
-
promoting Traditional Chinese Medicine (TCM);
-
free treatment abroad by Chinese doctors.
The BRI framework document The Belt and Road Initiative – Progress, Contributions, and Perspectives (April 2019) refers to 56 bilateral health agreements that China has concluded, inter alia with the WHO and the Bill & Melinda Gates Foundation. The BRI Standardisation Action Plans of 2015–2017 and 2018–2020 also mention Chinese efforts to set uniform standards for TCM and the definition of medical terms. The BRI Development Plan for Promoting TCM (2016–2020) makes it clear that Beijing plans to promote traditional Chinese medicine internationally.
In realising the Health Silk Road, as in all other areas of the BRI, Beijing acts strategically, flexibly and at several levels simultaneously (bi- and multilateral, regional, and global). The so-called China+x mechanisms are essential here. These are formats for Chinese cooperation, for instance with countries from the Association of Southeast Asian Nations (ASEAN) countries, Africa (FOCAC), Central and Eastern Europe (17+1), or the Arab League. Health cooperation within these mechanisms does present differences from region to region, but it reflects large swathes of the content (at times verbatim) of the Chinese BRI documents.
Since 2015 there has been a regular forum of the Chinese health minister with 17 (until 2019: 16) Central and East European colleagues (2015 in Prague; 2016 in Suzhou; 2017 in Budapest; 2019 in Sofia). The declared objectives of the format are the promotion of TCM in Europe, programmes for exchange and cooperation (for hospitals, the health industry, and universities), access to markets (for example for medicines), and cooperation in combating infectious diseases like MERS and SARS (see the Suzhou Declaration of 20 June 2016). New structures have been created for this format, including the 17+1 Hospital Alliance, the 17+1 Cooperation Network for Public Health, the 17+1 Cooperation Network for Health Workers, the 17+1 Research Network for Health Policy, and the 17+1 Cooperation Forum for Approval of Medicines.
Health was already a prominent part of China’s relationship with the ASEAN countries before the BRI was announced. In 2012 the parties concluded a Memorandum of Understanding on health cooperation. On 26 October 2016, the participants in the first China-ASEAN Health Cooperation Forum adopted the Nanning Declaration. It focuses on exchanging information, jointly preventing and controlling infectious diseases, training health sector professional, promoting TCM, and deploying Chinese doctors. For the “Lancang-Mekong” countries (Cambodia, Laos, Myanmar, Thailand, and Vietnam), one focus of China’s BRI health diplomacy is on free eye operations.
In September 2015 the China-Arab States Health Cooperation Forum was held as part of a dialogue forum that China has established with Arab League countries. According to the Yinchuan Declaration that it adopted, this cooperation includes technological collaboration, promoting TCM, preventing and controlling infectious diseases, medical training programmes, coordinating public health system reforms, exchanges between medical establishments and staff, and coordinating on global health issues.
Health cooperation is most significant in China-Africa relations, where it dates back to long before the BRI was announced (for example, the deployment of medical personnel, a decades-old practice). Since 2015 it has been absorbed into the BRI as part of the Forum on China–Africa Cooperation (FOCAC). It consists, inter alia, of providing medical supplies, training programmes, building hospitals, and support for combating infectious diseases such as malaria and Ebola (see e.g. the FOCAC Johannesburg Action Plan [2016–2018] and the FOCAC Beijing Action Plan [2019–2021]).
Health was also important within the BRI on a bilateral level before the Covid pandemic. China has been sending medical personnel to offer free treatment in regions where China+x formats are less widespread. Here China’s commitment in South Asia and Oceania must be emphasised (Beijing has sent teams of doctors to Nepal, Micronesia, Vanuatu, Tonga and Fiji, for example). China is also active in Central Asia. Its most important pilot project is the Medical Services Centre of the BRI Core Region Xinjiang. This hospital cooperation platform provides medical help for patients from neighbouring countries (such as free heart operations for Afghan children). It also aims to network Central Asian hospitals with Xinjiang (for example for medical tourism).
Most important at the global level is the Memorandum of Understanding on Health Sector Cooperation under the Belt and Road Initiative signed by China and the WHO on 18 January 2017. It uses the term Health Silk Road for the first time. The WHO’s explicit support for the BRI reflects the growing influence of the People’s Republic within the WHO, which has been noticeable for years. In August 2017 officials from many countries, international organisations and non-governmental organisations (NGOs) signed the Beijing Communiqué on BRI Health Cooperation and the Health Silk Road, which summarises the fundamental elements of China’s BRI health policy.
Activating the BRI Networks as Part of “Mask Diplomacy”
Once the coronavirus outbreak in Wuhan became known, China initially appealed to the international community and received material and financial aid from more than 58 countries (including Australia, Belarus, Djibouti, Germany, Pakistan, Bahrain, the USA and Surinam). Even smaller contributions (for instance a €100 donation from Comoros) were used for propaganda by Beijing as a sign of solidarity and evidence of the Health Silk Road mentality.
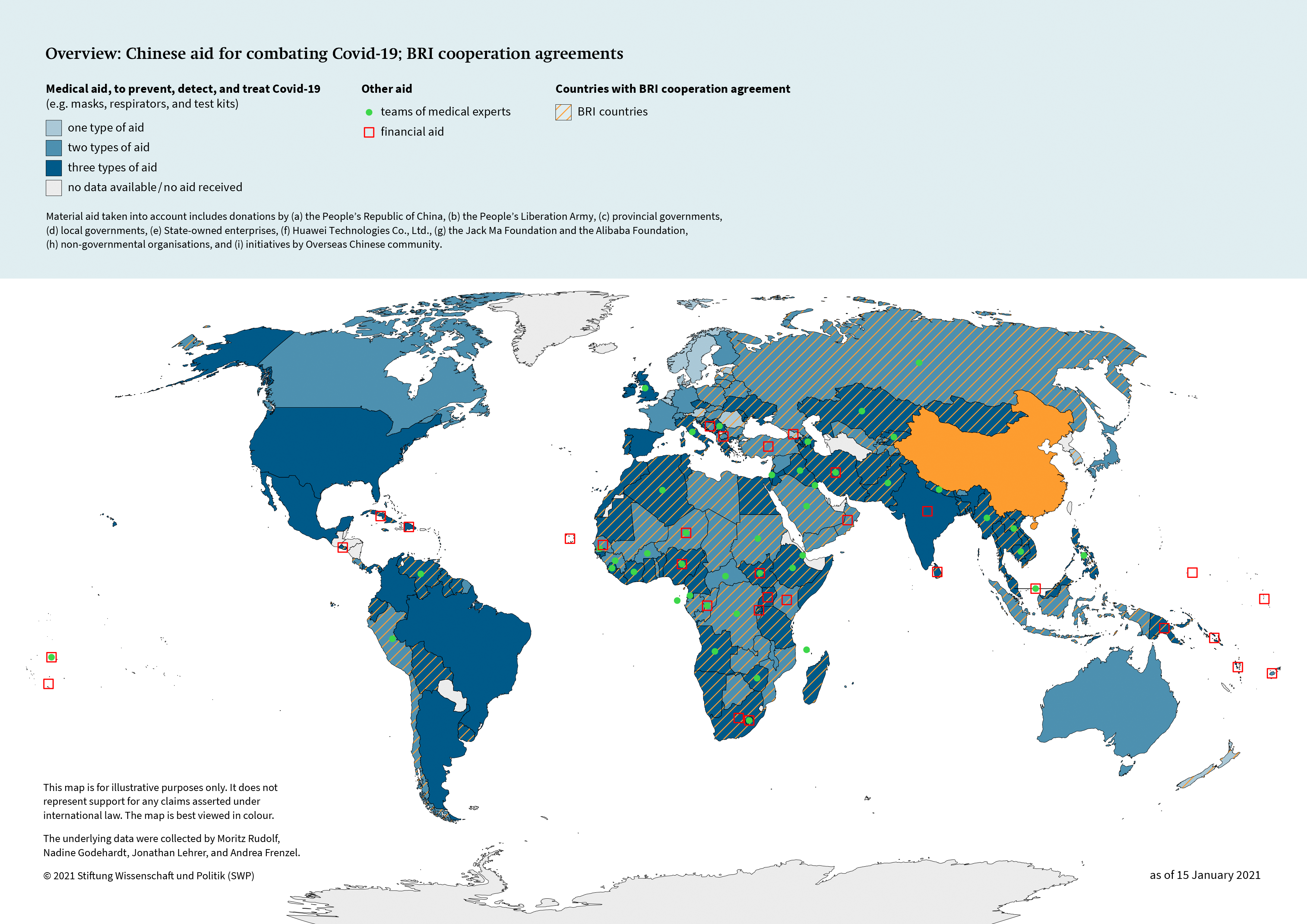
In late February, when the Chinese leadership had gradually regained control of the outbreak in the country, Beijing quickly took on the role of relief supplier. Since a majority of the world’s mask factories are in China and many industrialised nations had delivered relief aid to Wuhan, the Chinese leadership was in an almost monopolistic position to provide the world with masks and medical kits. In particular, countries that had inadequate medical equipment very quickly received donations of much-needed aid supplies (masks, test kits, and respirators). Beijing also sent teams of doctors to 43 countries. Nearly all the world’s countries have received support from China (see Map 1, p. 7).
Aid supplies came from a variety of actors, not only from China’s central government and the Communist Party, and often took into account China’s strategic interests in the recipient nation. Provinces and cities supplied their partner municipalities and regions. Majority Muslim countries (such as Afghanistan, Egypt, Iran, Iraq, Lebanon and Jordan) received masks from Xinjiang Autonomous Region. In Southeast Asia (e.g. Laos, Cambodia, Myanmar), soldiers from the People’s Liberation Army delivered medical aid supplies. In countries where Chinese state-owned companies run BRI projects (for instance in Africa), donors included relevant banks, construction companies, and raw material companies. The telecoms company Huawei preferentially gave support to countries in which it was pursuing strategic interests in the 5G expansion: in Europe these included the Czech Republic, Ireland, Italy, Lithuania, the Netherlands, Poland, Romania, Serbia, and Spain. Business foundations (especially the Jack Ma Foundation and the Alibaba Foundation) delivered masks, respirators, and testing apparatus to over 150 countries. Trade associations, overseas Chinese, and NGOs were also involved. As part of “mask diplomacy”, many recipient countries saw the involvement of locally resident Chinese actors, who normally tend to live apart in parallel societies. These forms of help for the local population correspond to the objective formulated in many BRI documents of generating broad support for China’s Silk Road policy.
China even offered aid supplies to states that do not (yet) have diplomatic relations with Beijing, especially in Latin America. In Paraguay the parliamentary opposition demanded that relations with Taiwan be broken off so as to receive aid from Beijing. Belize received donations of auxiliary materials from Chinese organisations that were supposedly NGOs. A remarkable PR coup for Beijing were the photos of Belize City councillors posing in front of Chinese flags.
China’s propaganda machine has been running at full speed for months. The content for this streamlined Covid-19 narrative comes from the white book Fighting Covid-19: China in Action. Chinese diplomats have been publishing articles in local daily newspapers in which they describe China’s relations with the country to which they have been posted according to this narrative. These articles present China as a rescuer that is the equal of the aid recipient countries, and as a responsible international great power. China’s help, the narrative claims using a key BRI expression, is symbolic of the “global community of common destiny” to which it aspires. The articles are reminiscent of China’s propaganda strategy in the early days of the BRI: similarly, back then sizeable newspaper adverts were used (though primarily by members of the leadership, not diplomats) to promote the BRI.
A new development is China’s presence on “Western” social media such as Twitter or Facebook, which are not available in China. Almost every day, China’s diplomatic missions disseminate updates on social networks about China’s local contributions to combating Covid-19. Xi Jinping’s wife, the singer and WHO special envoy Peng Liyuan, also has a role in China’s health diplomacy, for instance by leading online ceremonies to mark Chinese assistance. Peng has also personally donated protective masks to many African countries.
China’s mask diplomacy has been criticised, particularly in Europe; the necessary logistics, activation of Chinese actors, and uniform external communications are nevertheless remarkable achievements. For many countries China was a reliable partner, especially since traditional aid donors (above all the USA) were absent. For the first time, Beijing has given its global BRI rhetoric some substance.
Next Act: Vaccination Diplomacy
Phase III trials are currently running in 18 countries, especially in Latin America, Southeast Asia, and the Arab world, for the vaccines produced by five Chinese companies (Sinopharm, CanSinoBIO, Sinovac and Anhui Zhifei Longcom Bio, IMBCAMS). China has already concluded contracts for vaccine deliveries with 26 countries; 10 (see Map 2, p. 8) have approved Chinese vaccines (as of 18 January 2021). Many other countries would like to use a Chinese vaccine or are currently negotiating contracts.
On this issue, too, the Chinese leadership wants to be perceived as a “responsible great power”. Once again it is acting bi- and multilaterally. On 18 May 2020 Xi Jinping announced in a speech to the WHO in Geneva that China would be providing the world with an inexpensive vaccine as a “global public good”. This is typical BRI rhetoric. The Initiative has been promoted using the same vocabulary for years. President Xi also promised the WHO US$2 billion for the fight against corona. In October Beijing joined the vaccine platform COVAX, an initiative by the United Nations, European Union and France, which aims to ensure a fair distribution of vaccines.
While the first months of the pandemic were marked by bilateral aid supplies, Beijing has been increasingly using China+x formats for its vaccine diplomacy. These formats link vaccine promises with the prospect of economic support and long-term cooperation projects. The starting-point was the Extraordinary China-Africa Summit on Solidarity against Covid-19 (June 2020). The Chinese leadership promised preferential vaccine deliveries, “debt cancellation”, and reinforced economic relations after the pandemic (such as help with investments in the digital economy, boosting renewable energies, and expanding the 5-G network). One month later, Beijing organised a health summit with the Arab League states. Here too China held out the prospect of vaccination cooperation as well as strengthened bilateral economic relations (under the BRI framework). Also in July, Beijing promised Latin American and Caribbean countries US$1 billion for purchasing vaccines. On 24 August Prime Minister Li Keqiang explained that the Lancang-Mekong countries would be prioritised for vaccine deliveries and that funding could come from a Public Health Fund. In turn Foreign Minister Wang Yi identified the ASEAN as a priority region for vaccines. Similar promises (vaccine priority and expansion of economic relations) were made at the China-Pacific Island Forum. In November high-ranking officials from China and South Asian countries (Bangladesh, Nepal, Pakistan, Sri Lanka) held talks about vaccinations.
What is remarkable is that the most advanced format institutionally, the 17+1, has played a subordinate role in China’s vaccine diplomacy. In 2020 only two webinars were held at vice-ministerial level. China’s vaccine diplomacy in Europe, on the other hand, has been designed bilaterally and is aimed primarily at Hungary and Serbia.
China’s commitment to Latin America and the Arab world is particularly prominent. These regions have recently also gained importance for the BRI. The new China-Pacific Islands health cooperation forum in turn emphasises China’s strategic orientation towards the southern Pacific.
Assessment
The BRI has not floundered on Covid-19, as some observers had predicted in the early days of the pandemic. On the contrary, Beijing has increasingly been linking its contribution to combating the pandemic with the BRI narrative (e.g. the advantages of global connectivity; the construction of a “global community of common destiny”). With its high degree of flexibility, strong political will, and logistically advantageous starting position, the BRI has so far been able to weather the test of this crisis.
Beijing’s health diplomacy has revealed the way the initiative functions, and especially its adaptability. Virtually overnight, health was promoted from a marginal to a key subject of the BRI. In the briefest of times, China activated BRI networks around the world. The necessary infrastructure was already available from other BRI components. BRI rail links and the so-called Air Silk Road (with hubs in Luxembourg and Liège) were repurposed as supply lines for aid goods. Now the interlinking of the Digital Silk Road with the health BRI is also on the agenda (for instance to facilitate contact tracing). Institutionally China can here draw on numerous China+x mechanisms to drive the BRI forward.
While, in the early days of the pandemic, the USA mostly did not participate in international aid measures, China filled this gap and is now advancing further into the traditional backyards of the USA’s spheres of influence (Latin America and the Arab world).
The widespread view in Germany and Europe that China’s mask diplomacy has been unsuccessful, fails to recognise that China has been targeting success in countries outside of Europe, where it is increasingly viewed as a responsible great power. Beijing has been helping third states effectively and extensively.
After the pandemic, China might well be able to further expand its influence in key BRI regions: it has been acting strategically and far-sightedly in its (health) initiative. Its health diplomacy links measures to combat the pandemic with BRI promises (prosperity through connectedness with China). To counteract further growth of China’s influence on strategic regions, Europe should make proposals to third countries for the post-pandemic period (political cooperation and economic support). Europe has a lot of catching-up to do in this respect. Its understanding of the geopolitical implications of Covid-19 is insufficient.
Chinese competitors have so far not emerged as forerunners in the vaccine race. Yet there are promising Chinese vaccines. Despite growing doubts over their efficacy, Beijing will profit from national production capacities in the coming months and be in a position to provide the Global South with vaccines. Beijing plans to vaccinate 50 million of its own citizens against the coronavirus by early February. It would not be surprising therefore if Chinese vaccination teams were deployed in developing nations in the coming months under the BRI banner.
Political decision-makers in Germany and Europe need to realise and react to the fact that China’s health diplomacy, just like the entire BRI, operates on several levels simultaneously: bi- and multilateral, regional, and global. Multilateral commitments (e.g. within the WHO) should be strengthened; where appropriate, China should be cooperated with (for instance under COVAX). However, this alone is insufficient. Over the past few years, Beijing has massively expanded China’s influence at the multilateral level (especially within the WHO). To oppose this expansion in third countries, Germany and Europe would do well to strengthen their own bilateral commitments as well. Regional EU+x formats with countries in strategically relevant regions (e.g. Indo-Pacific or Africa), or appropriate measures coordinated with the new Biden administration in the USA, would be potential courses of action.
Moritz Rudolf is an Associate in the Asia Research Division at SWP.
© Stiftung Wissenschaft und Politik, 2021
All rights reserved
This Comment reflects the author’s views.
SWP Comments are subject to internal peer review, fact-checking and copy-editing. For further information on our quality control procedures, please visit the SWP website: https://www.swp-berlin.org/en/about-swp/ quality-management-for-swp-publications/
SWP
Stiftung Wissenschaft und Politik
German Institute for International and Security Affairs
Ludwigkirchplatz 3–4
10719 Berlin
Telephone +49 30 880 07-0
Fax +49 30 880 07-100
www.swp-berlin.org
swp@swp-berlin.org
ISSN 1861-1761
doi: 10.18449/2021C09
Translation by Tom Genrich
(Updated English version of SWP‑Aktuell 5/2021)