Regional Health Care in the EU
ESI Funds as a Means of Building the European Health Union
SWP Research Paper 2024/RP 01, 12.01.2024, 49 Pagesdoi:10.18449/2024RP01
Research AreasMichael Bayerlein is an Associate in the EU / Europe Research Division at SWP. He works on the project “The Global and European Health Governance in Crisis”, which is funded by the German Federal Ministry of Health (BMG).
-
This research paper examines the role of the European Structural and Investment (ESI) funds in building the European Health Union (EHU) in the context of the mid-term review of the multiannual financial framework and the high variance in excess mortality during the Covid-19 pandemic.
-
It provides a detailed analysis of the determinants of regional excess mortality and investigates how ESI funds can contribute to building the EHU and resilient health systems through cohesion funding and the convergence of living conditions.
-
It focuses on verifying three hypotheses derived from the literature: (1) economic deprivation and differences in medical infrastructure influence excess mortality; (2) ESI funding leads to an improvement in medical infrastructure; (3) ESI funds support the development of resilient health systems.
-
The results show that economically disadvantaged areas were hit harder by the pandemic and that ESI-funded regions show positive developments in their medical infrastructure.
-
ESI-funded regions have lower excess mortality than comparable regions. This only applies, however, to regions which had experienced a positive economic development in the context of the funding.
-
Alongside ESI-supported economic development and the improvement of medical infrastructure, there must be capacity-building specifically for fighting dangers to health.
-
This research paper recommends using ESI funds to enhance resilience, taking economic determinants into account, and distributing health resources equitable. Building the EHU will thus require an across-the-board approach that combines ESI funds with other initiatives.
Table of contents
2 Building a Health Union for the EU
3 A Cartography of the Pandemic
3.1 European Regions and Rural Areas
3.2 The Economic Determinants of Health
4 Health-related Disparities in the EU
4.1 Determining Regional Differences
5 Determinants of Covid-19 Excess Mortality in the EU
5.1 An Overview of Influencing Factors
5.2 Empirical Analysis of the Determinants
6 Strengthening the Regions Using ESI Funds
6.1 Criteria for Cohesion Funding
6.3 The Indirect Influence of ESI Funds
6.4 Further Funds to Enhance Health Care
7.1 Measuring the Effects of ESI Funds
7.2 Improving Medical Infrastructure
7.3 Building Resilient Health Systems through ESI Funding
7.4 Successful Funding of Regions
Issues and Recommendations
In 2023 the EU Commission launched the mid-term review of the multiannual financial framework. In its submission, the Commission will also position itself on the future use of ESI funds. It is already becoming clear that it considers the funds less and less as a means for cohesion funding and creating equivalent living conditions but rather increasingly as an instrument for strengthening regions that are already prospering. Simultaneously, targeted funding via the EU Recovery Fund and the European “Green Deal” are gaining in importance vis-à-vis cohesion funding. However, the Covid-19 pandemic in particular has shown that the EU is only as strong as its weakest regions. There were substantial differences in excess mortality between member states, but it is the great variance within member states that deserves attention above all.
The very fact that the excess mortality in rural areas in later phases of the pandemic exceeded that in urban centres demonstrates the regional inequalities within EU member states. In this context, and with a view to the European Commission’s declared objective of building a European Health Union (EHU), this paper will address two questions. How can regional differences in excess mortality during the Covid-19 pandemic be explained? And how can public health disparities be overcome within the framework of EU governance?
To answer these questions, the paper will examine three hypotheses: (1) The factors that determine subnational variance in excess mortality are regional economic deprivation and differences in the regional medical infrastructure, primarily the number of hospital beds and available medical doctors. (2) The European Structural and Investment (ESI) funds are able to contribute to improving regional medical infrastructures. (3) ESI funds support the creation of resilient health systems that enable member states to face future disease outbreaks.
These three hypotheses are derived from a range of research contributions. Previous studies have already analysed the effects of ESI funds on regional economic development, political views and electoral behaviour. They have especially highlighted the positive economic impact of ESI funding. By contrast, research into regional differences in the public health system is still scarce, especially in the context of the Covid-19 pandemic and the creation of the EHU. Nonetheless, the few studies have already shown that ESI funding in earlier funding phases successfully contributed to closing gaps in access to health care and in public health research and potentially also supporting the construction of the EHU.
That a robust EHU needs to be established was highlighted not least by the pandemic. This necessity is a result particularly of the asymmetry between economic and health integration in the EU. While the EU has few legislative competences in health policy, the free movement of people, goods and services is associated with the challenge of facing cross-border health threats – or rather, preventing them from developing. Here, both public health and health care are crucial. The EHU addresses both aspects; however, its competence base is weak.
Given the creation of the EHU and the potential reorientation of the EU’s cohesion policy, it is important to understand how excess mortality during the pandemic was linked to regional health inequalities, and to what extent these regional differences are also based on economic determinants of health. Conclusions can be drawn from the findings of this paper on the role that regional ESI funding has or could have in building the EHU. The other factors associated with excess mortality in addition to regional health inequalities and economic determinants of health are examined in detail in the study and their influence is statistically controlled.
The results show that regional economic deprivation is a decisive factor in explaining the differences in excess mortality during the Covid-19 pandemic that were observed both between and within EU member states. The analysis further demonstrates that this identified economic deprivation partly coincides with medical infrastructure deficiencies and especially with poorer overall population health. It also shows that the EU’s cohesion policy is associated with an improvement in regional medical infrastructure. However, this improvement has not led to a reduction in excess mortality in the funded areas vis-à-vis comparable regions without funding. Rather, only those areas registered lower excess mortality in which regional funding was followed by corresponding economic growth. Moreover, this paper’s case study concludes that the lack of specific regional capacities for fighting health threats as well as insufficient investment in the health system are also associated with higher excess mortality.
These findings suggest that the fundamental regional economic development as well as improved medical infrastructure are essential components in building the EHU. However, investment in the medical sector beyond medical infrastructure and the equitable distribution of countermeasures in a crisis are also important. In building the EHU, the EU’s cohesion policy should therefore continue to be a priority, in combination with other initiatives for strengthening health care and public health within EU member states.
Building a Health Union for the EU
For the EU and its member states, the Covid-19 pandemic highlighted the existing deficiencies in the health care infrastructure and underscored the deficits in fighting public health threats. However, these deficits were known before the pandemic and are often attributed to “constitutional asymmetry”1. This expression describes the fact that the EU has, on the one hand, a high degree of integration and competences in economics, but on the other hand almost no competences in welfare-state redistribution or health care, despite the latter being necessarily connected to the former.2 Moreover, the legal and economic framework for integration further restricts the room for manoeuvre of member states’ welfare systems.3 The result is far-reaching integration of the European economy but, simultaneously, insufficient expansion of comprehensive and robust public health and health care.
Commission President Ursula von der Leyen’s announcement in her State of the Union address 2020 of the creation of an EHU4 can therefore be interpreted as a reaction to this asymmetric integration, which the pandemic highlighted so clearly. The aim and purpose of the EHU is to better protect the health of EU citizens; to enable the EU and its member states to prevent and combat future pandemics more efficiently; and to reinforce the resilience of European health systems.5 These objectives refer both to public health and to health care. The latter encompasses medical infrastructure and access to health services, while public health means combatting communicable and non-communicable diseases.6 This differentiation is relevant because the EU’s competences in the two areas are markedly different. Essentially, its competences in both areas are relatively limited under Articles 4 and 6 of the Treaty on the Functioning of the European Union (TFEU). Article 168 para 7 TFEU assigns the competence for population health care entirely to the member states.
The EHU objective of building more resilient European health systems can therefore not be met through legislation. Rather, the EU will have to resort to other governance mechanisms to overcome existing deficits and the above-mentioned constitutional asymmetry and improve national health systems. In this regard, EU funds that co-finance projects in members states and thus create incentives for investment in various areas are key elements. With the help of these instruments, the EU could especially contribute to improving health care at the regional level and thus promote the cohesion of its regions.
Strengthening the ability of EU regions to face future health threats is closely linked to the issue of existing deficits. Only once these weaknesses have been identified can the EU and its member states set priorities and use means accordingly. This research paper examines the health deficits that emerged in the EU during the Covid-19 pandemic to examine the role of ESI funds in building the EHU. The pandemic is suitable for this approach in two respects. First, it provides the opportunity to identify weak points in the resilience of health systems. Second, it can also be seen as a natural experiment that makes it possible to evaluate pre-pandemic policy measures in terms of their impact on public health and the resilience of healthcare systems. Early analyses have already shown the existence of substantial differences in how hard the Covid-19 pandemic hit member states as well as individual member state regions.7 However, the identification of determinants of excess mortality within the EU is still patchy. As a consequence, the first issue tackled by this research paper is how to explain the regional differences in the impact of the Covid-19 pandemic. It will then analyse the political project of the EHU and the role of ESI funds. This requires a cartography of the pandemic and an examination of individual determinants.
A Cartography of the Pandemic
Excess mortality is a frequently used measure to determine how badly affected countries and regions were by the pandemic. The World Health Organization (WHO) defines excess mortality as "the mortality above what would be expected based on the non-crisis mortality rate in the population of interest.”8 Excess mortality is thus the mortality that can, with high probability, be ascribed to crisis conditions. It can be expressed as a rate (the difference between the observed mortality and the average mortality before the crisis event) or as the total number of excess deaths. As a rate, excess mortality captures the difference in the number of deaths in a selected area or time period as a percentage deviation from the expected number of deaths.9
Using excess mortality rather than the actual number of Covid-19 deaths has the advantage that the severity of the pandemic becomes comparable across different moments in time and regional contexts, since testing and reporting capabilities would otherwise substantially distort the comparison of Covid-19 related deaths.10 Excess mortality figures also log increased mortality due to illnesses which are not related to Covid-19 but which can equally be attributed to the health systems’ overload during the pandemic.11 However, using excess mortality to capture the regional impact of the pandemic presumes that total mortality has been correctly reported and that the number of deaths that are not related to the pandemic remains stable.12 The last assumption can be violated at times, since measures to restrict mobility, such as lockdowns and quarantine requirements, can for example have an impact on traffic-related deaths. Regardless of these limitations, this research paper will use excess mortality to determine the regional severity of the pandemic since it remains the indicator best suited for assessing how hard the pandemic hit various countries and regions. In particular, it makes comparing different territorial units possible.
European Regions and Rural Areas
The Covid-19 pandemic impacted countries all over the world to differing degrees. Studies analysing European countries have already shown that there was often great variance in the excess mortality rate both between countries and within the countries themselves.13 A useful source for analysing excess mortality during the pandemic is the European Commission’s 8th Cohesion Report, which documents the regional dimension of the Covid-19 pandemic.14 Figure 1 is based on the report’s approach and shows the excess mortality in the three regions –the Northern and Western, Southern and Eastern Europe – in the years 2020 and 2021.15
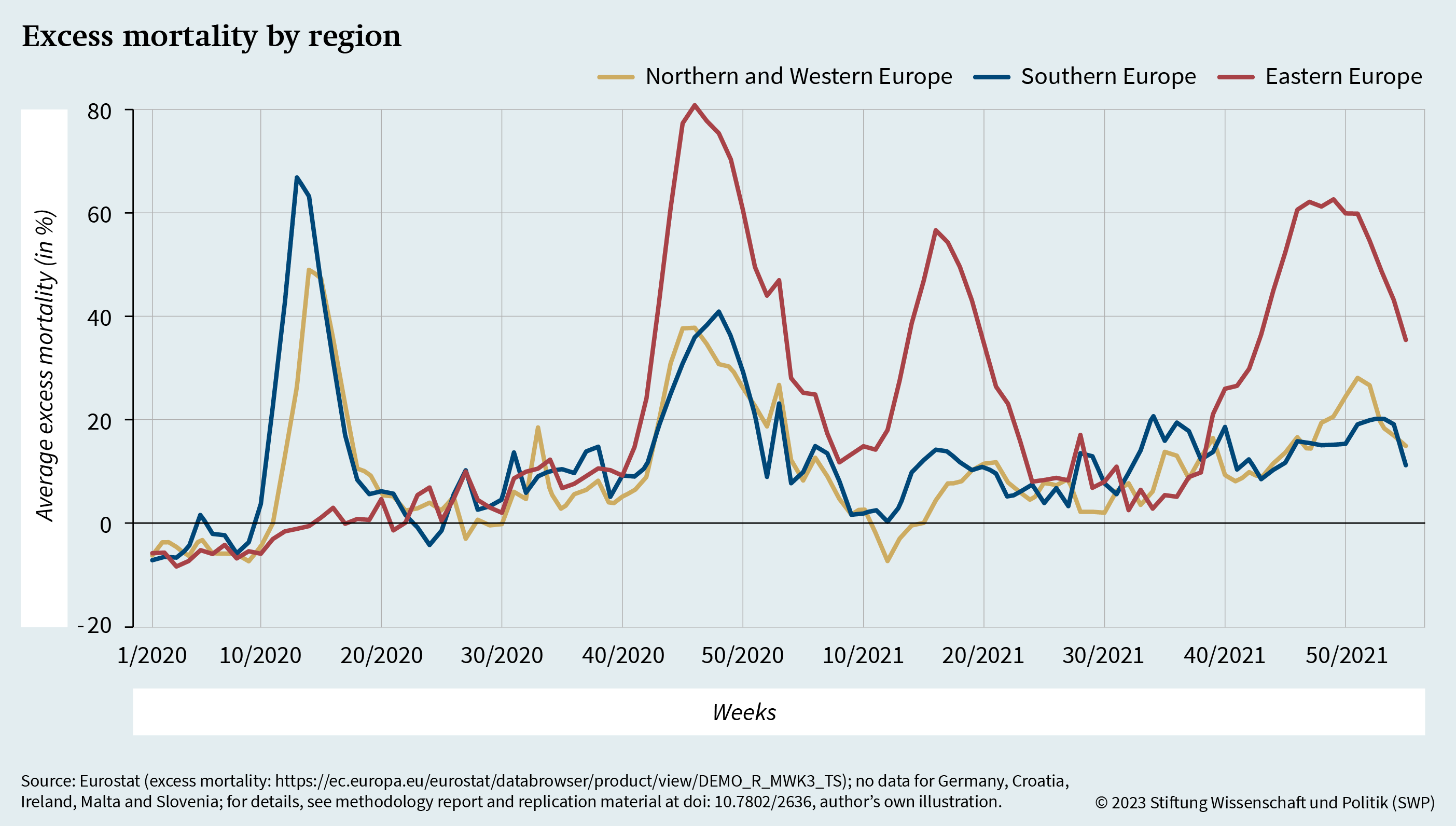
As the figure shows, the pandemic initially peaked in Southern Europe between the tenth and 20th week of 2020 and, with a slight delay, in Northern and Western Europe. While the second wave, in the winter of 2020, was associated with a renewed increase in excess mortality in Northern and Western Europe as well, the figure indicates above all a dramatic rise in excess mortality – to a maximum of 80 per cent – in Eastern Europe. Similar spikes can also be seen there during subsequent waves, in the early summer and winter of 2021. In comparison, excess mortality in Northern and Western Europe remained relatively low at the same time. The final wave of the winter of 2021 is also remarkable: vaccination campaigns had been up and running in all EU member states for up to a year.
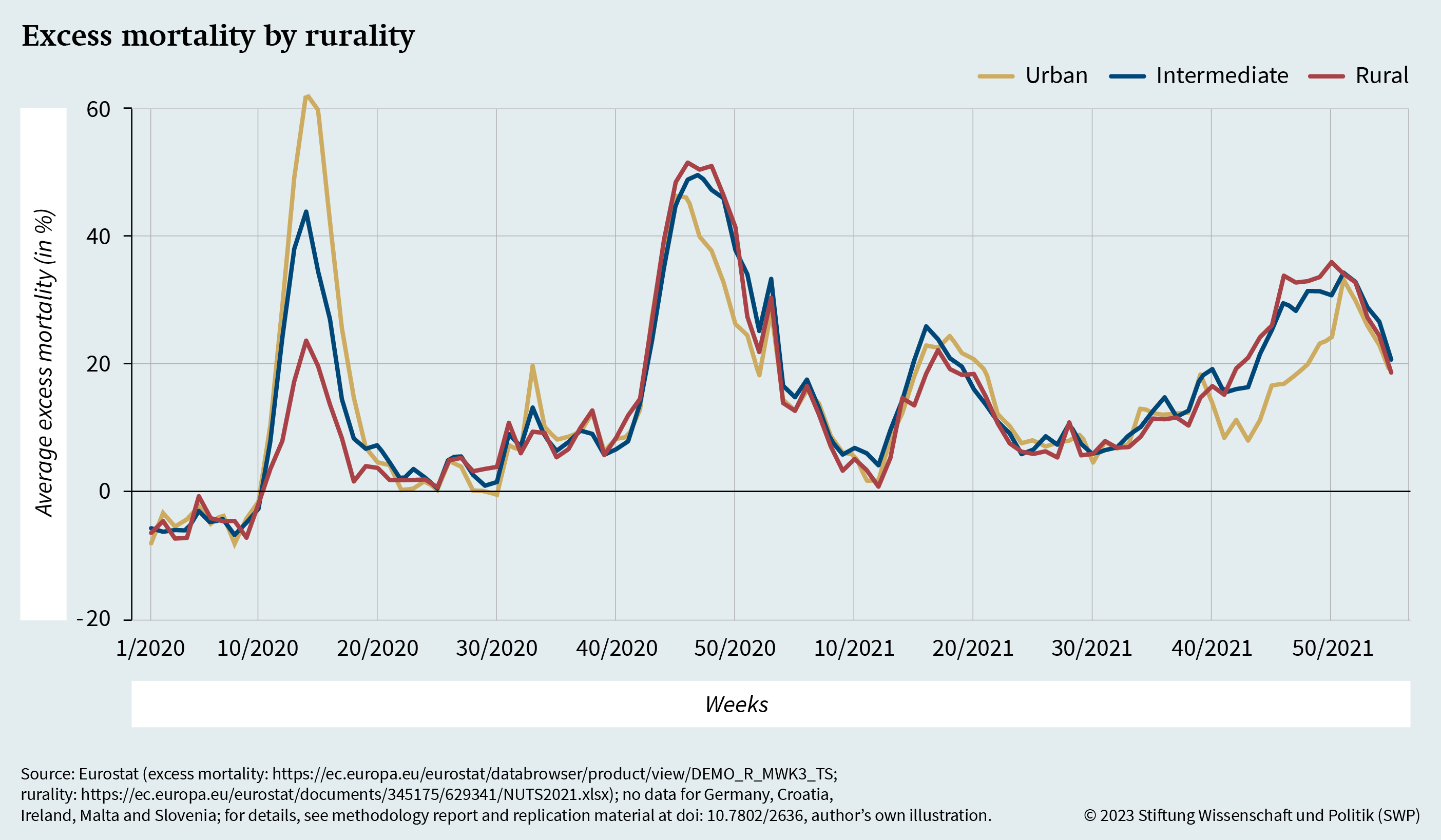
The issue is how to explain the outlined regional differences in excess mortality. The European Commission’s 8th Cohesion Report specifically addresses the differences in excess mortality between urban and rural areas. Figure 2 shows this difference using the EU typology, which differentiates between urban, intermediate and rural territorial units (NUTS-3 regions).16
The figure has a clear peak between the 10th and 20th week of the year 2020 for all three regions. This peak in excess mortality is most marked in urban areas, followed by intermediate and rural areas. Research has found that the higher infection rates and associated increase in excess mortality in the EU’s urban centres were reflected in other countries, which displayed a similarly strong correlation between highly populated areas and Covid mortality.17 In later waves, however, rural and intermediate areas caught up: in the second wave of winter 2020, both types of areas had slightly higher excess mortality, a difference that was even more pronounced in autumn 2021. While the conclusion can be drawn that in its later phases the pandemic expanded to a certain extent to rural areas,18 no substantial distortion at the expense of rural areas can be made out in the pandemic’s later phases. Therefore, differences in excess mortality cannot solely be explained by the rurality of regions but are more likely to be rooted in structural characteristics sometimes associated with rurality.
To determine any connection between rural areas and excess mortality and bring out the structural characteristics which contribute to higher excess mortality, Figure 3 presents excess mortality at the regional level in relation to the respective population density.
The map uses dark red to show higher excess mortality at lower population density and dark blue for higher population density with lower excess mortality. Dark purple indicates areas with high excess mortality and high population density. Figure 3 clearly shows the above-described differences between and within EU member states: Southern European member states such as Spain, Greece and Italy and above all Eastern European countries such as Poland, the Czech Republic, Bulgaria and Romania have a markedly higher excess mortality than member states like Germany, Sweden and Finland. The map illustrates not only the differences between the countries but also the clear subnational clusters in all member states. While these clusters are often correlated with higher population density, i.e., with urban areas, there are also several clusters that are not linked to densely populated areas. These regions are coloured red and have a high rate of excess mortality at low population density.
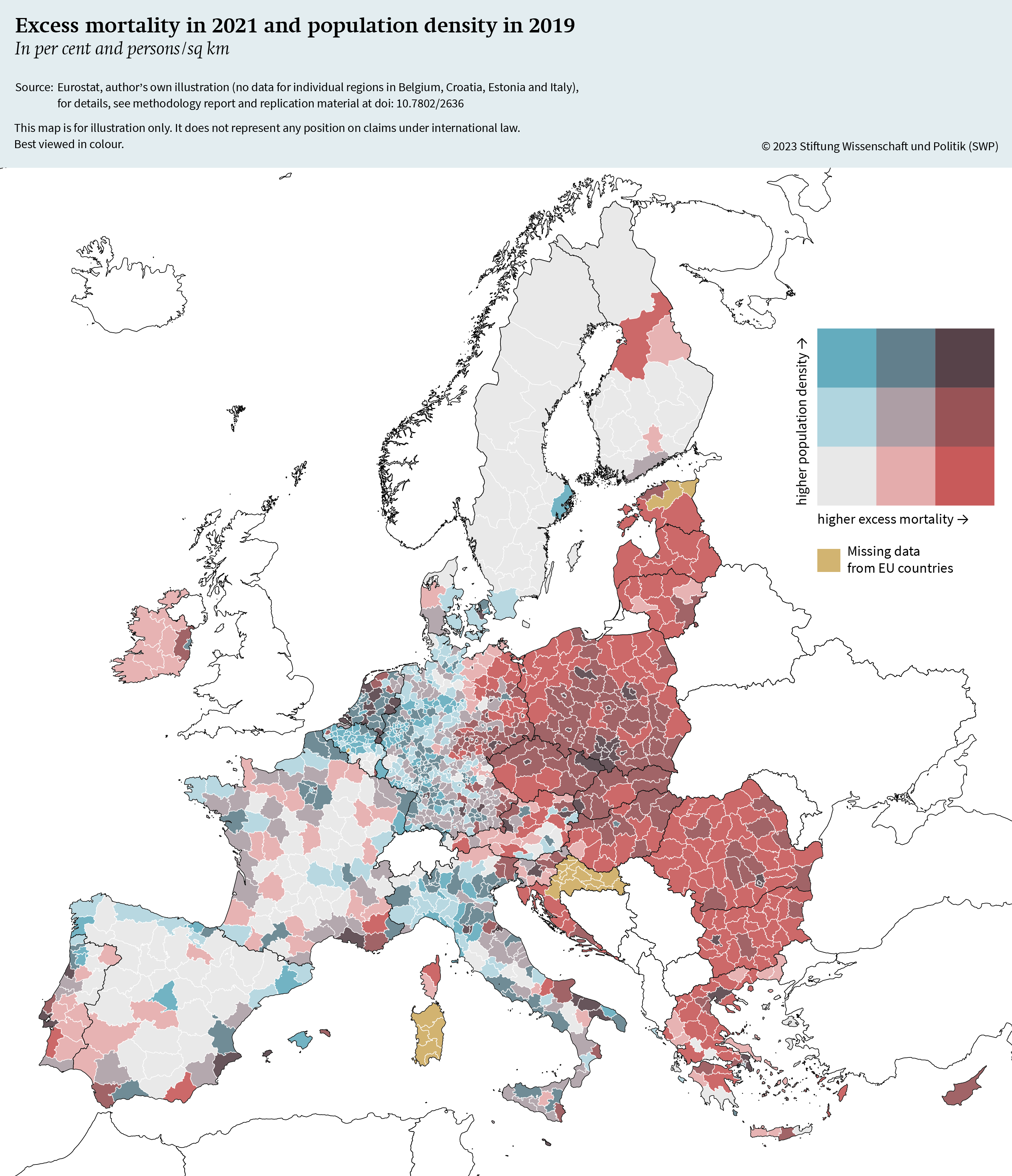
The map thus demonstrates that subnational variance can partly be attributed to higher excess mortality in thinly populated regions. Simultaneously, some urban areas display low rates of excess mortality; others, however, do not.
From this follows that the simple distinction between urban and rural areas should be discarded so that potential structural determinants of higher excess mortality can be linked to specific regional characteristics in the EU.19 Earlier studies have shown that poverty increased the impact of the pandemic on excess mortality in French municipalities due to its association, for example, with places of work with higher risks of exposure and crowded living conditions.20 Similarly, densely populated and marginalised communities in Mexico City had higher excess mortality during Covid-19.21 These observations also coincide with research results from Chile, which show that very crowded living conditions are positively correlated with excess mortality while higher levels of education are negatively correlated with excess mortality.22 The analysis of all EU member states also suggests that there is a connection between regional economic development and excess mortality while no influence of individual poverty could be established.23 Research findings from European and non-European countries thus indicate that economic disadvantages and deprivation can cause higher excess mortality. This is consistent with the discovery that, in later phases of the pandemic, rural areas occasionally showed higher rates of excess mortality since rurality is often associated with economic disadvantage.
The Economic Determinants of Health
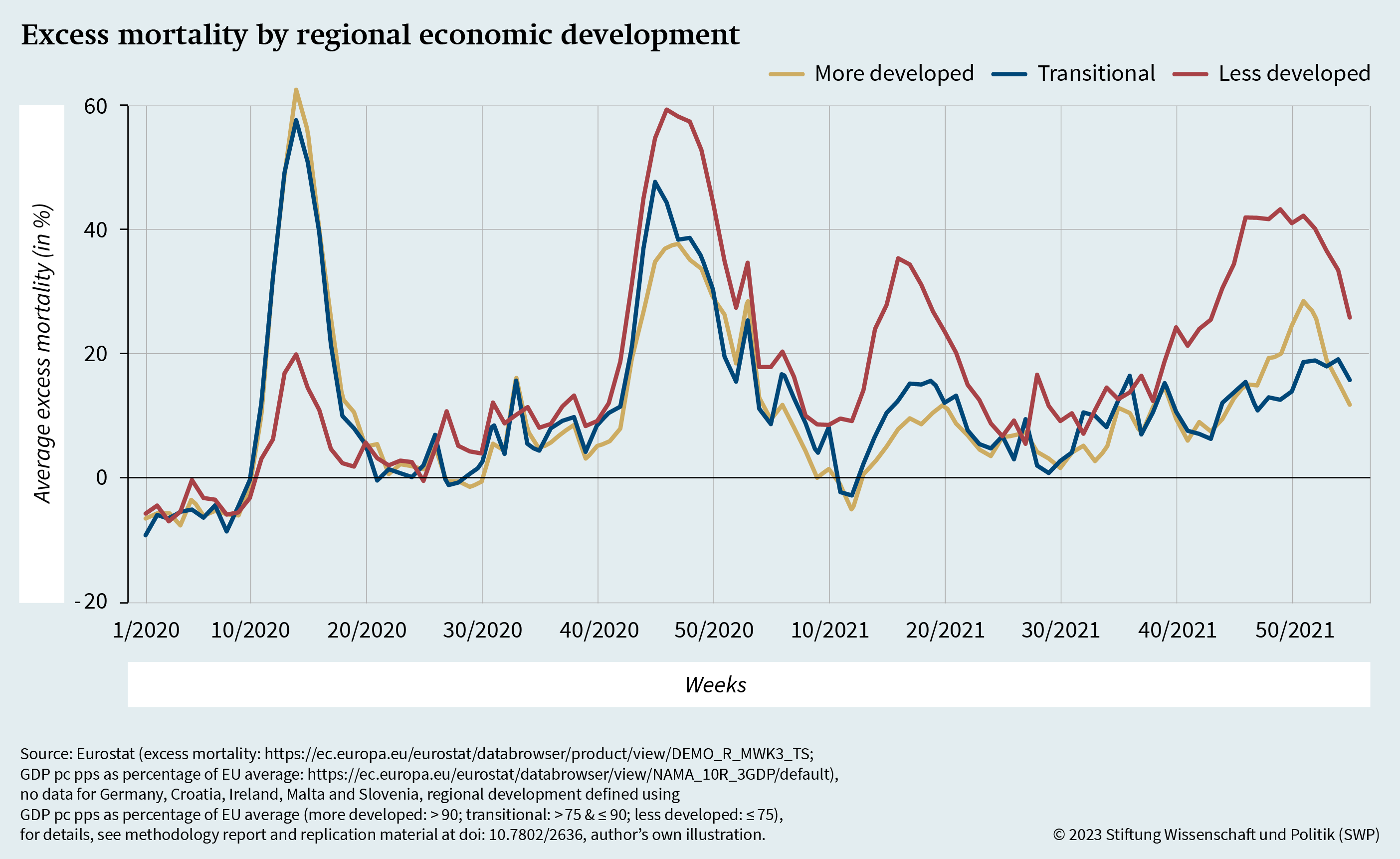
According to the analysis, Southern and Eastern EU member states – and to certain extent rural areas in all EU member states – had particularly high excess mortality in later phases of the pandemic. A possible reason could be the weaker economic development of these regions. Figure 4 explores this assumption by comparing the excess mortality of European regions according to the economic-development typology used in the allocation of ESI funds. In the funding period 2014 to 2020, this typology differentiates between “more developed”, “less developed” and “transition regions”.
The definition of a “less developed” region is one which has a per capita (pc) gross domestic product (GDP) expressed in purchasing power standard (pps) that is lower than or equal to 75 per cent of the EU average. Regions with values between 75 and 90 per cent are categorised as “transition regions”, regions with values above 90 per cent as “more developed”.24 Figure 4 shows clear differences in excess mortality depending on economic development. The progression of the pandemic coincides with the previous findings, whereby it first impacted urban regions and increasingly also the economically more developed regions in Northern and Western Europe, while subsequent waves laid bare deficits in the health systems of the rural and economically less developed areas of Eastern Europe. This concurs with the finding that, in the first six months of the pandemic, economic disparities were not significantly associated with excess mortality.25
In sum, this section provides evidence on the determinants of the variance in excess mortality that existed between and within EU member states. Later phases of the pandemic showed a disparity between Northern and Western EU member states on the one and Southern and Eastern EU member states on the other side. This gap partly runs along an urban-rural axis. However, it is not rurality itself that is associated with higher excess mortality. Rather, in later phases of the pandemic it is differences in regional economic development that codetermines the variance in excess mortality between and within EU member states.
In their analysis of overall structural factors such as rurality and economic disadvantage, studies have also emphasised the role of health infrastructure, which is one factor that explains the differences in excess mortality during the Covid-19 pandemic both between countries and within countries. Disparities in health infrastructure are generally linked to the economic disadvantage of areas. These inequalities have an immediate effect, for instance a lack of hospital beds and medical doctors fundamentally compromises population health and additionally endangers care in crisis situations. The next section will therefore describe disparities in public health and health care in the EU and put them in the context of the excess mortality that has been identified.
Health-related Disparities in the EU
Naturally, health-related disparities in the EU already existed before the Covid-19 pandemic. They concern both regional inequalities in public health and differences in medical infrastructure between and within the member states. Both components in turn had an effect on regional excess mortality during the Covid-19 pandemic, as outlined above.
Apart from the medical infrastructure, socio-economic determinants play an important role in health-related disparities within the EU. These encompass economic factors in the sense of regional and individual economic capacities as well as social factors such as education, social capital, individual employment circumstances and discrimination. Studies have shown that a lower socio-economic status is correlated with both reduced life expectancy and increased risk of illness.26 Earlier research even found that the health-related disparities between European countries were continually growing,27 while more recent findings indicate that the gaps between countries are on average at least not widening, although health disparities dramatically increased within certain population groups in Eastern Europe.28
Determining Regional Differences
While health-related disparities exist in the Northern, Southern, Western and Eastern Europe, average life expectancy in individual Eastern EU members states is markedly less stable and overall significantly lower.29 This fact can be attributed to long-standing socio-economic differences between the regions, which were reinforced by the economic transformation that followed the collapse of the Soviet Union.30 Alongside these developments, there are also subnational inequalities in the Eastern European countries caused by socio-economic factors such as economic disparities or unhealthy lifestyles, which are associated especially with non-communicable cardiovascular diseases.31
With reference to the inequalities described in the literature, Figure 5 shows the average life expectancy in the three EU regions. The previously discussed differences between the Eastern European countries and the other two EU regions are pronounced and tally with previous findings.
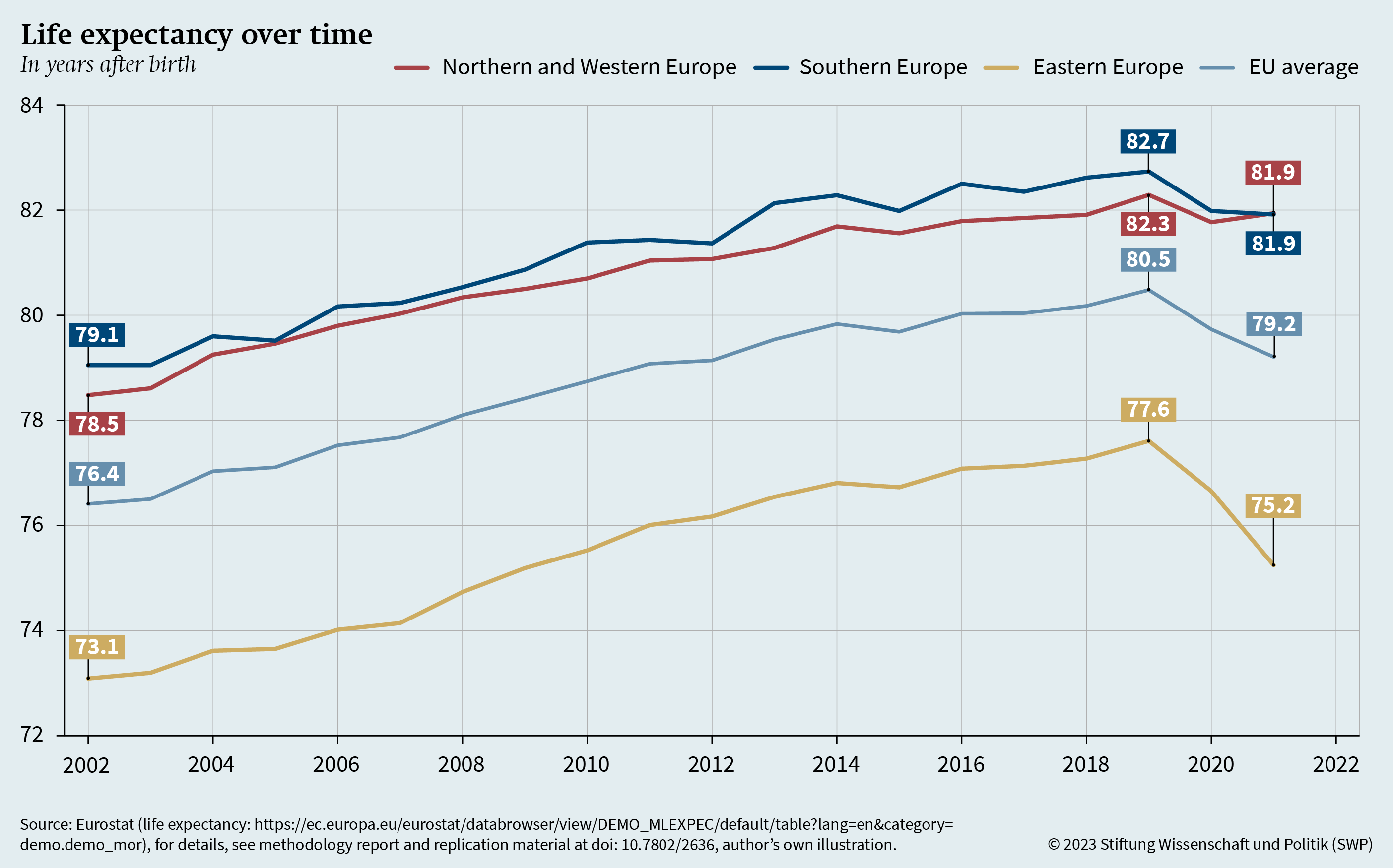
One conspicuous point is the stable difference in life expectancy, which has only decreased from about six years to five years from 2002 to 2019.32 The figure also clearly shows that, over the course of the Covid-19 pandemic, life expectancy in the Eastern Europe dropped much more sharply than in Northern and Western or Southern Europe. In the latter regions, life expectancy stabilised again in 2021 whereas it collapsed further in Eastern Europe.
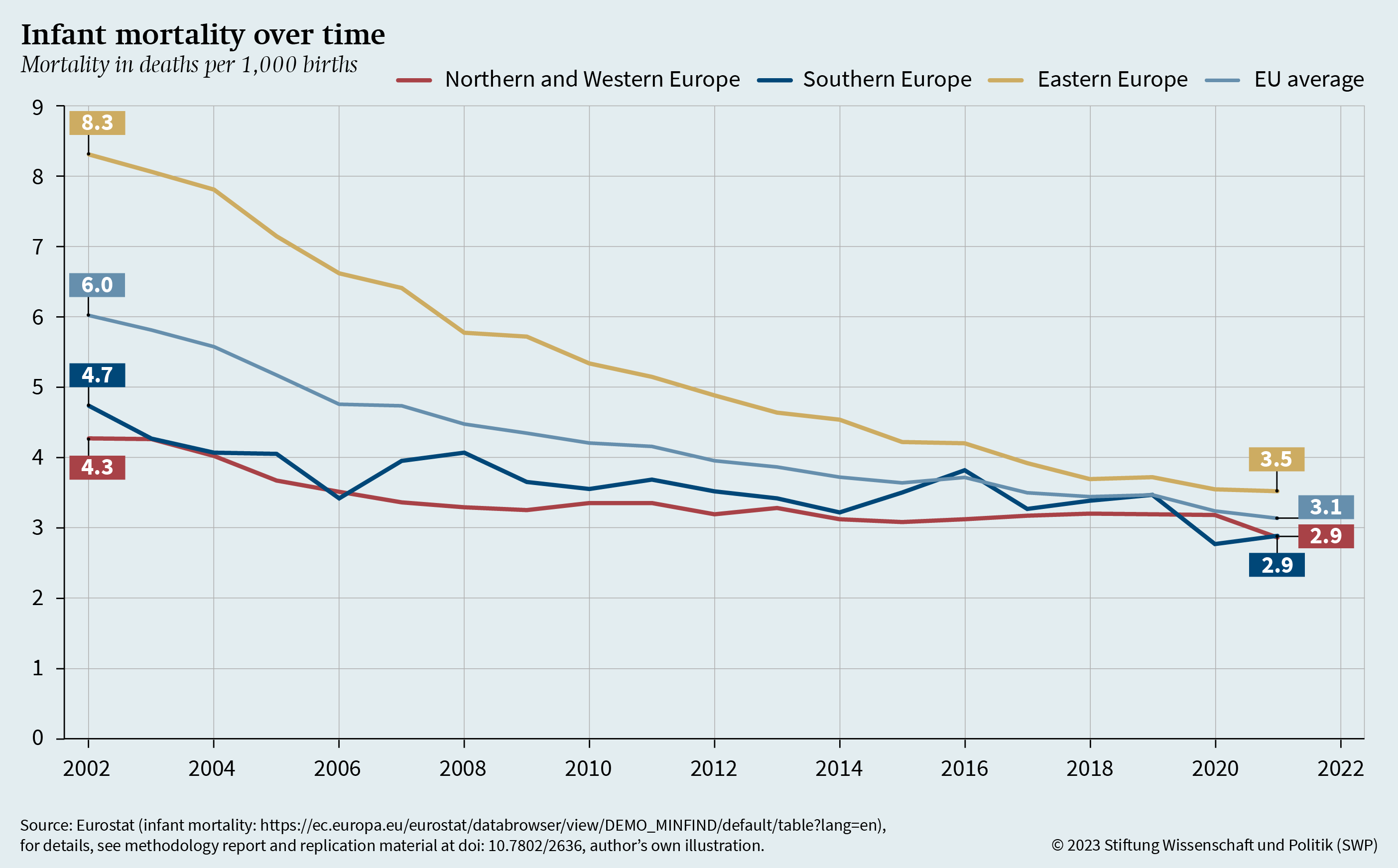
Beyond this, however, differences in health care and medical infrastructure are also relevant. Alongside life expectancy, infant mortality is a common measure to determine the quality of health systems and population health care. Figure 6 shows the corresponding values in the EU.33
The figure shows a clear reduction in infant mortality in all three EU regions to a very similar level in 2021. This is remarkable in as much as infant mortality in Eastern Europe was still far higher in 2002 than in Northern and Western or Southern Europe. In other words, while there are marked differences in life expectancy, they are almost negligible in terms of infant mortality. The question is whether this finding can be explained by the medical infrastructure.
Medical Infrastructure
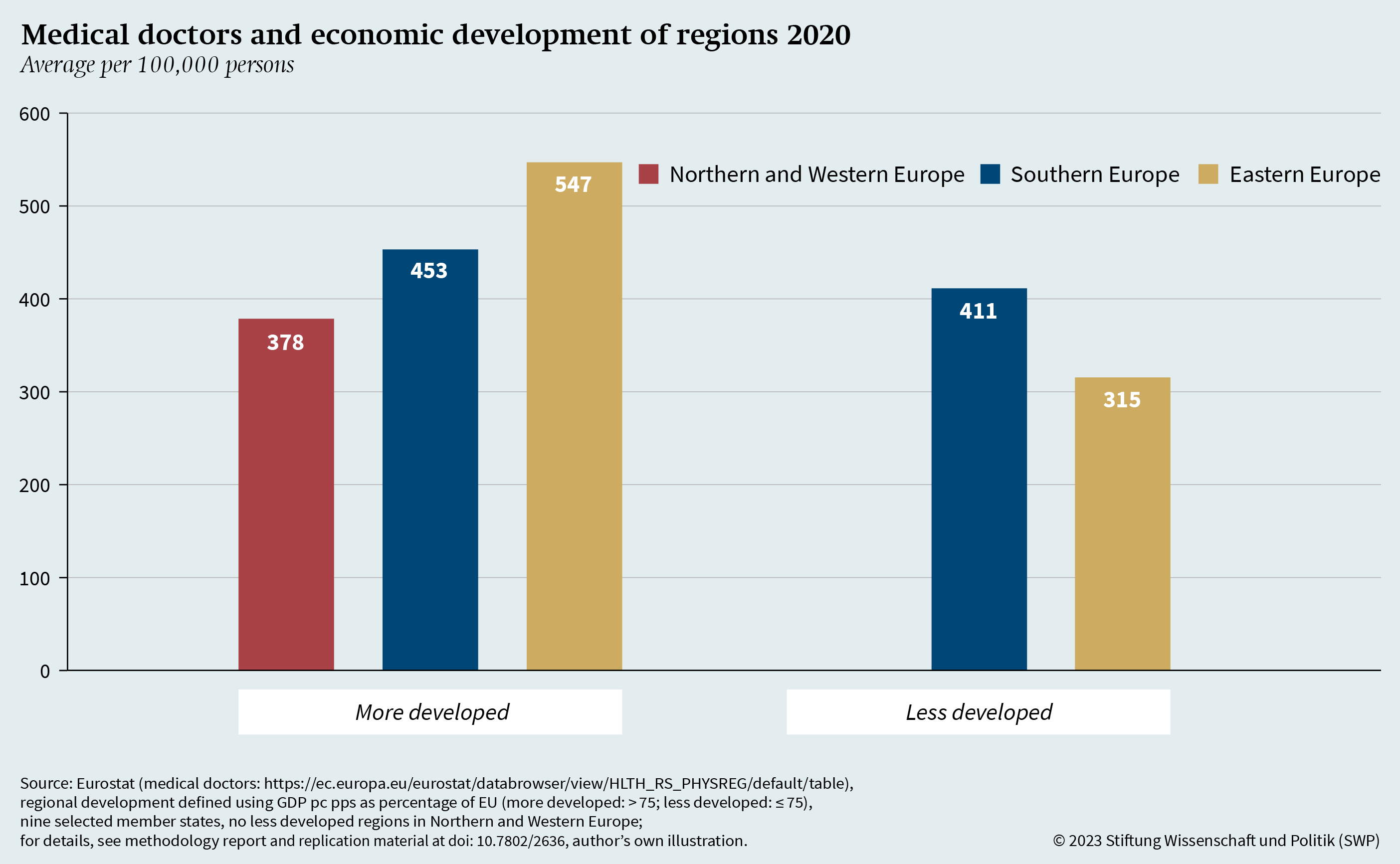
The Covid-19 pandemic put significant pressure on health systems in many EU member states, revealing existing inequalities.34 Even before the pandemic, there were marked differences within the EU in the distribution of hospital beds and medical doctors, mostly along geographical and economic divides.35 Focusing on differences in the medical infrastructure, Figure 7 shows the number of doctors per 100,000 inhabitants in 2020, divided into economically more developed areas (GDP pc pps of over 75 per cent of the EU average) and less developed areas (GDP pc pps equal to or less than 75 per cent of the EU average).36 It should be noted that there are no less developed areas left in Northern and Western EU member states.37
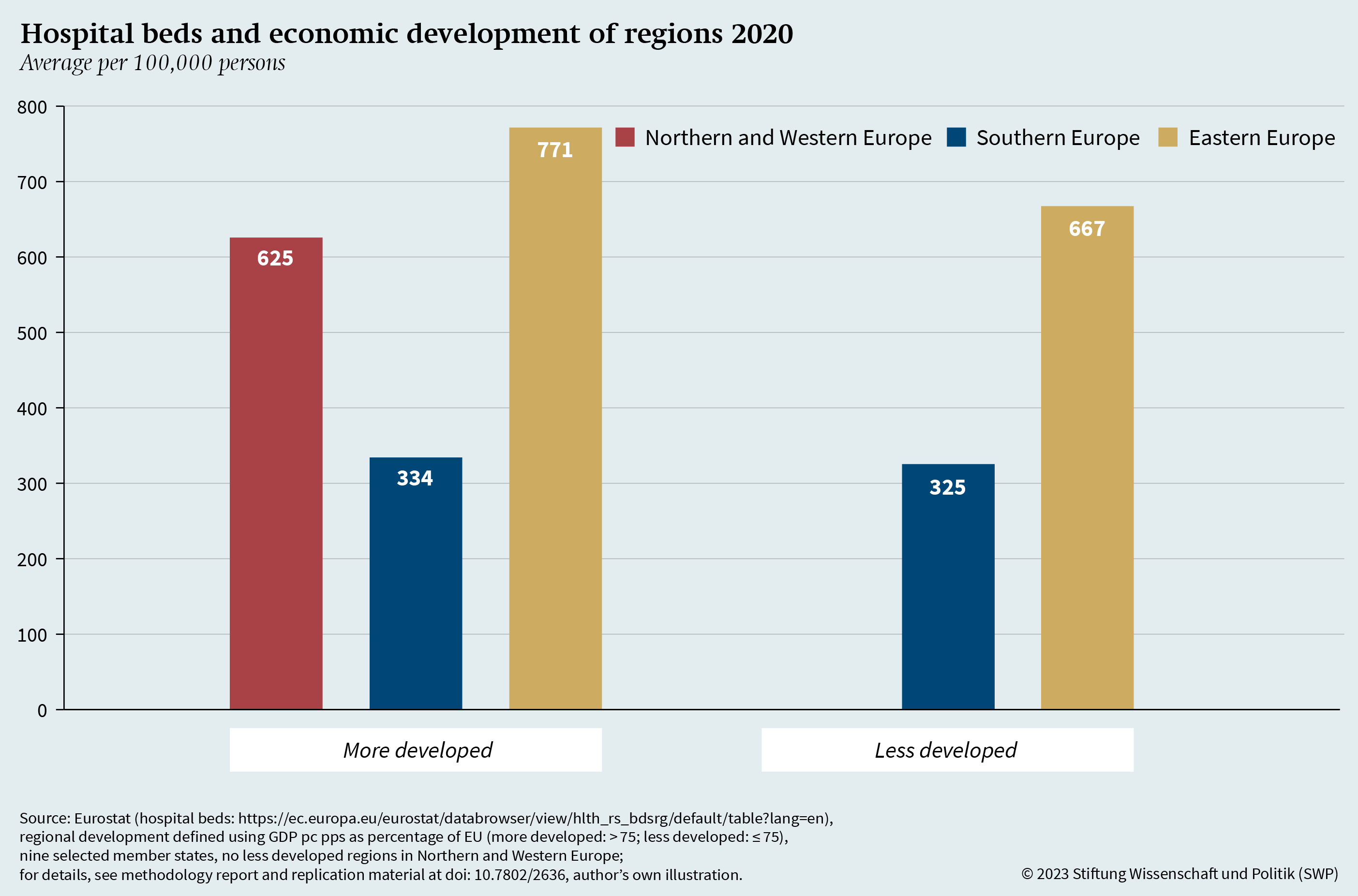
As the figure indicates, more developed regions have, on average, higher numbers of doctors than less developed regions. The difference between more and less developed regions is statistically significant in Eastern Europe. In contrast, in Southern Europe no significant difference can be identified. While these findings partly replicate insights from earlier research,38 the picture is slightly different regarding the distribution of hospital beds. Figure 8 shows this distribution for 2020, differentiating once again between more and less developed regions and between the Northern and Western, Southern as well as Eastern European member states.39
According to the figure, the less developed regions have slightly lower numbers of hospital beds than the more developed regions. These differences are peculiar in two ways. First, they are significant in neither the Southern nor Eastern Europe, unlike the differences in medical doctors. They do not correlate with an economic axis either but follow a geographical differentiation instead: Northern and Western as well as Eastern EU member states versus Southern EU member states. Second, as illustrated by the figure, the number of hospital beds in eastern EU is on average about twice that in Southern EU and even exceeds that in Northern and Western EU member states.
In sum, the analysis uncovered some differences in the medical infrastructure between the European regions. For medical doctors, there is a differential between economically more and less developed regions, which is particularly marked in Eastern Europe. However, the situation is not the same for hospital beds. The only significant difference here is between Southern European regions and the rest of the EU. This means that no clear differentiation of medical infrastructure can be established based on regional development. One might conjecture therefore that there is no link at all between economic development and medical infrastructure. In that case, the excess mortality in regions would exclusively be caused by general economic deprivation and the other determinants of Covid-19 excess mortality. To confirm or refute this hypothesis, other influencing factors – such as age, population density, vaccination rate, trust in the government, health spending and educational level – must be included in the analysis, and the reciprocal impact of medical infrastructure, economic development and additional determinants must be considered. Only this will make it possible to determine the effect of individual factors more precisely.
Determinants of Covid-19 Excess Mortality in the EU
Many studies have explored the issue of determinants that might explain the differences in excess mortality in the populations of individual countries or regions during the Covid-19 pandemic. Alongside different forms of governance and governments’ political orientation,40 they have above all highlighted structural factors.41 More recent contributions transcend political and institutional structures and point out, in line with the findings presented above, that especially at the start of the pandemic globalised and more developed areas were harder hit. Their higher population density42 and better transport links43 facilitated the spread of the virus, leading to a substantial increase in the number of infections and thus also of deaths.
An Overview of Influencing Factors
While the Covid-19 pandemic in the EU started in urban centres, infections shifted from the urban and more developed centres to rural and less developed areas in winter 2020 at the latest.44 Especially in the later phases of the pandemic, research has identified regional economic disparities,45 fundamental socioeconomic deprivation46 and the quality of health care47 as being relevant determinants of excess mortality. However, it also discusses many other factors that might be associated with higher excess mortality. These include pollution and air quality,48 population age,49 vaccination rates,50 political trust,51 the individual’s assessment of the political reaction to the crisis,52 national capacities for fighting health threats,53 an individual’s ideological position,54 education,55 chronical illnesses,56 unhealthy lifestyles57 and vaccination in previous waves.58 Due to this paper’s focus, this (incomplete) list of factors cannot be discussed in detail. The empirical analysis that follows does, however, take these determinants into account in analysing the correlation of economic development and medical infrastructure with regional excess mortality.
Empirical Analysis of the Determinants
From previous research, the hypothesis can be derived that regional economic deprivation and differences in the regional medical infrastructure – alongside other determinants – are decisive factors for explaining the subnational variance in excess mortality during the Covid-19 pandemic. To verify this hypothesis, the link between excess mortality on the one hand and economic deprivation and medical infrastructure on the other needs to be examined. In order to do so, subnational level (NUTS-2) data from Eurostat is employed. Since data are not available for all countries, the analysis is limited to nine EU members: Austria, Bulgaria, France, Hungary, Italy, Portugal, Romania, Slovakia and Spain. French overseas territories and Spain’s enclaves in Northern Africa have been excluded. In total, each of the three EU regions is represented at least twice.
The analysis encompasses 101 NUTS-2 regions of the nine states, using the most up-to-date data on medical infrastructure from the year 2020. It operationalises medical infrastructure with the number of doctors and hospital beds per 100,000 people in the respective area. To examine the correlation with excess mortality, the mortality data from 2021 are used. The previous year is unsuitable because when the Covid-19 pandemic hit in 2020 – especially in the first half of 2020 – no country was prepared, and richer regions registered higher numbers of cases because of their global exposure. This was mainly because little was known at the time about the pandemic and the virus.59
Excess mortality from 2020 is nevertheless taken into account in this analysis since immunisation and the loss of particularly vulnerable persons in the first waves condition excess mortality in subsequent waves.
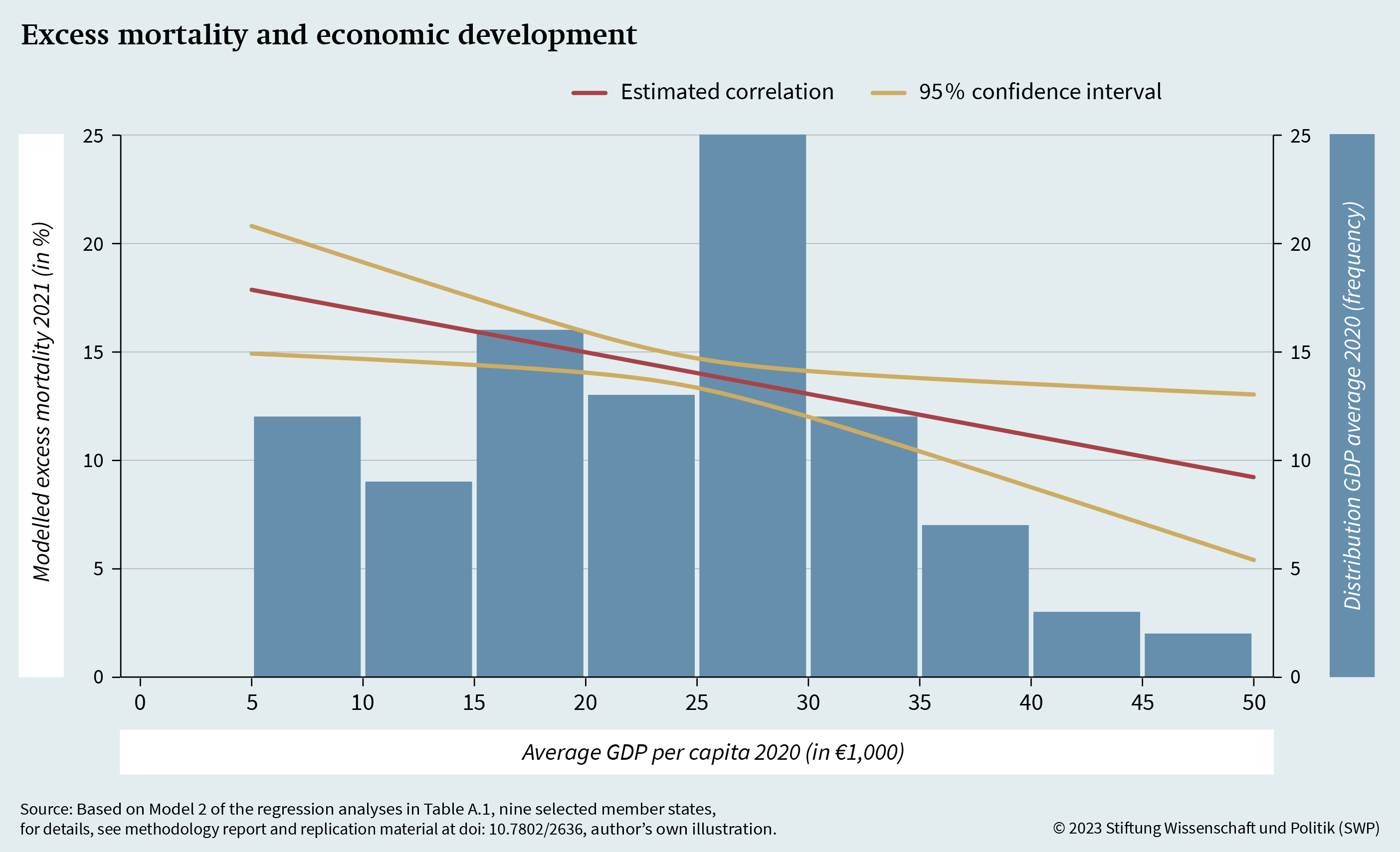
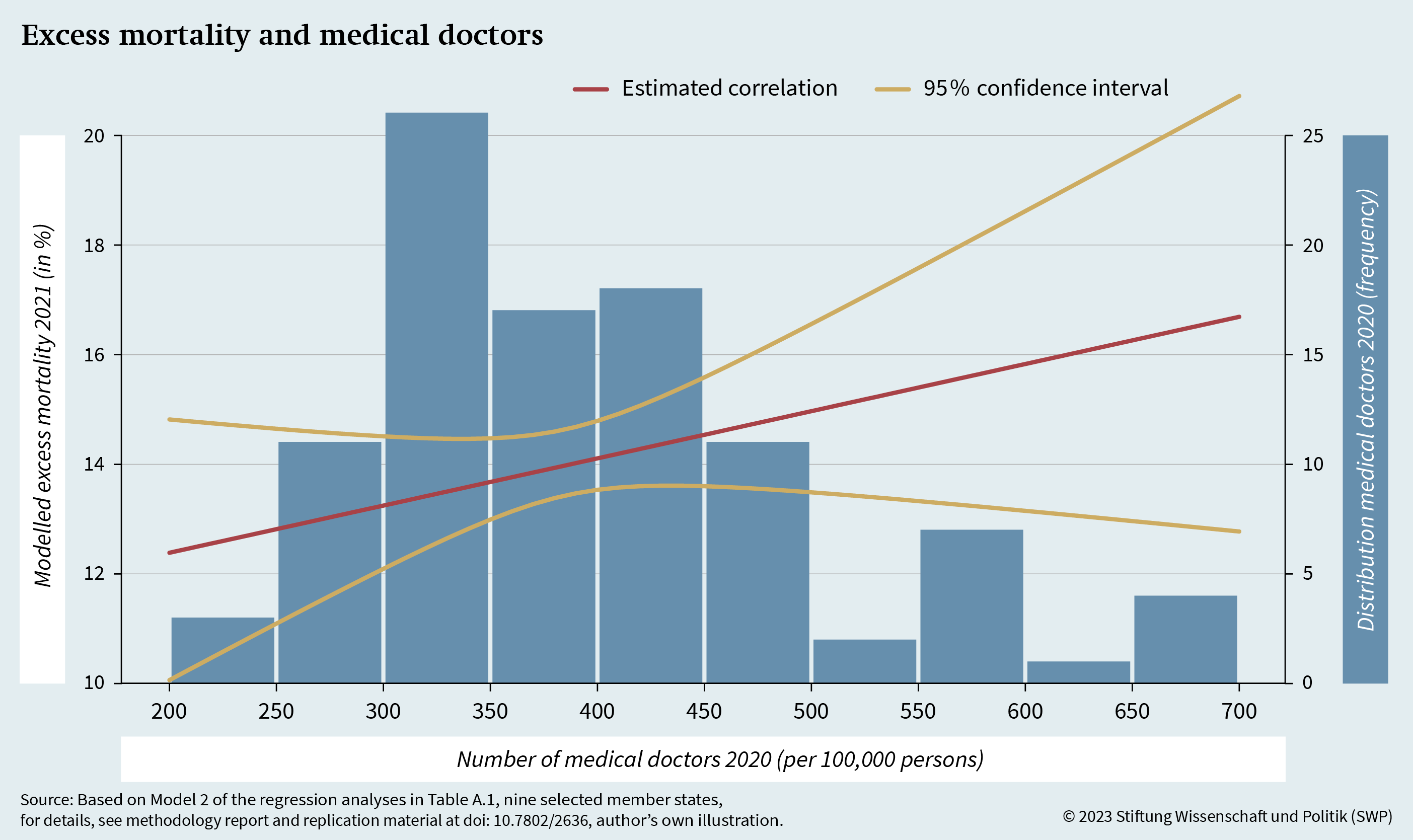
Figure 9 presents the model-based correlation between the regional density of medical doctors and the rate of excess mortality. The underlying statistical model describes the correlation between excess mortality and medical doctors, taking into consideration the additional determinants of regional excess mortality described above (see Table A.1). The figure indicates a weak positive correlation; however, it is not statistically significant. This also coincides with the bivariate correlation (see Figure A.1), which does not establish any significant association between excess mortality and medical doctors.
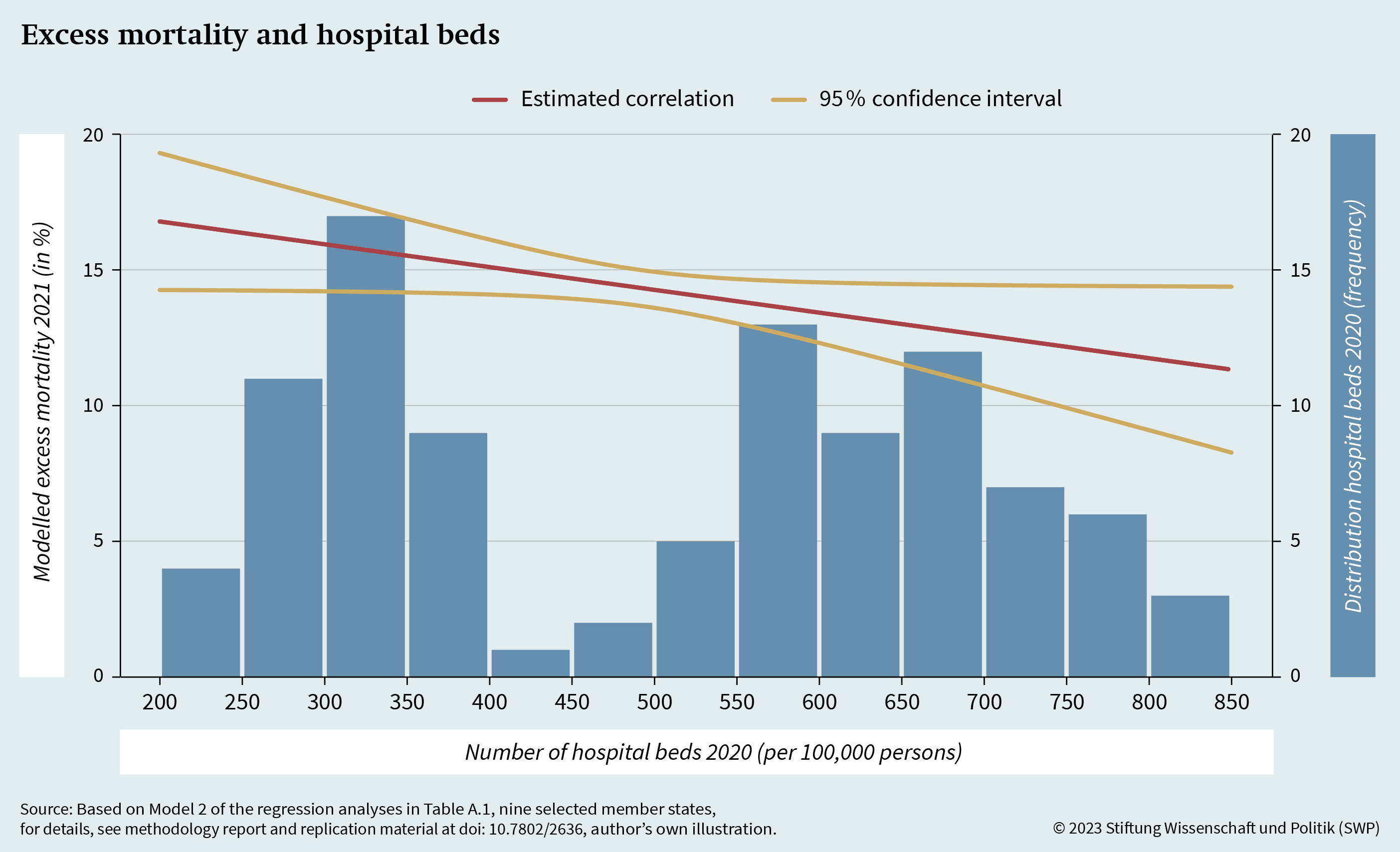
Figure 10 presents the modelled correlation between hospital beds and excess mortality at the regional level. Again, the model controls for other influencing factors. What is immediately striking is that the modelled correlation between the variables is clearly negative. This means that a higher number of hospital beds is correlated with lower excess mortality. While Figure 8 demonstrated that the number of hospital beds was not significantly correlated with economic deprivation, this model allows for the conclusion that NUTS regions with a higher density of hospital beds display lower excess mortality than similary regions with fewer hospital beds. Once again, this finding concurs with previous research.60 The analysis further shows that it is necessary to include control variables. Without them, the correlation is initially positive (see Figure A.2), which is contradictory and does not coincide with research findings on the effect of hospital beds.
The analysis of the key indicators for medical infrastructure and health care thus gives a mixed picture. While no significant association between medical doctors and Covid-19 excess mortality could be discerned at the regional level in the EU, the statistical model (that controls for other determinants) at least shows a negative and statistically significant correlation between the number of hospital beds and excess mortality in 2021. This is particularly evident when comparing similar regions that differ only in the density of hospital beds. The estimated excess mortality is significantly higher in areas with higher density than in lower-density areas, taking additional factors into account.
Finally, this study examines the economic determinants of excess mortality. For this, it uses the previously employed model to calculate excess mortality at the regional level based on the nominal GDP pc of the respective territorial unit. The results of the calculations are presented in Figure 11. The statistical analysis shows a robust negative correlation between the GDP pc of territorial units in 2020 and their respective excess mortality in 2021. This correlation remains significant even when controlling for regional medical infrastructure and the additional determinants of excess mortality described above. The purely bivariate association (see Figure A.3) is somewhat more quadratic, and robust across regions. A quadratic estimate was not used in the models since no distortion of estimation errors was observed in the linear modelling. In contrast with previous analyses, not only the model but also the bivariate analysis shows a negative and significant correlation.
While the literature also introduces additional structural and individual factors to explain the regional and subnational variance in excess mortality, this examination of territorial units of the selected nine EU member states concludes that economic deprivation in particular correlates significantly with this variance. In addition, a negative association with excess mortality was also found for the medical infrastructure in the form of hospital beds when controlling for other influencing factors. The same correlation was not found for medical doctors.
To summarise, the statistical analysis of the determinants of excess mortality suggests that the economic strengthening of regions should be accorded particular attention in building the EHU. Alongside this, the analysis uncovered a correlation between the expansion of medical infrastructure in the form of hospital beds and excess mortality; however, this relationship is much less pronounced than the economic relationship.
Strengthening the Regions Using ESI Funds
Strengthening the EU regions with the aim of creating equivalent living conditions is one of the core components of European integration and is expressed even in the EU treaties, for example in Article 174 TFEU. A key element that the EU can use to create equivalent living conditions are the five European Structural and Investment (ESI) funds.61 These are the European Regional Development Fund (ERDF), the European Social Fund (ESF), the Cohesion Fund (CF), the European Agricultural Fund for Rural Development (EAFRD) and the European Maritime, Fisheries and Aquaculture Fund (EMFAF).62 The ERDF and ESF are particularly interesting for cohesion policy, since they contain specific mechanisms for funding disadvantaged subnational territorial units (NUTS-2 regions). The two funds differ in their funding objectives. While the ERDF aims to strengthen economic, social and territorial cohesion by funding infrastructure projects, the ESF foregrounds labour market measures, which improve training or integration into the labour market and occasionally the recruitment of workers.
Criteria for Cohesion Funding
While all regions can in principle obtain funds from the ERDF and ESF, special funding exists for regions whose GDP pc pps is lower than 75 per cent of the EU average.63 However, the amount is not tied to the 75 per cent mark. The GDP per capita pps to determine the eligibility of a region is calculated based on a three-year average seven years prior to the start of funding. For the funding period 2007 to 2013, the base is the years 2000 to 2002,64 for the funding period 2014 to 2020, it is the years 2007 to 2009.65
The regions designated “less developed” qualify for the highest possible level of EU funding.66 In these cases, 85 per cent of the costs are co-financed by the EU; the ESI funds’ budgets are thus mostly used for cohesion and convergence funding.67 Eligible projects range from expanding infrastructure to transforming production and commercial sites to training courses that support integration into the labour market.68 The ERDF and ESF also encompass funding for projects to improve medical infrastructure, especially in Eastern Europe (see Figure A.4). Additionally, the European Commission explicitly calls for ESI funds to be used for medical infrastructure improvements.69 Possible objectives of projects include, for example, the expansion and transformation of medical centres and hospitals,70 the improvement of ambulance availability and patient transport services71 and the recruitment of specialist staff in towns or abroad.72
Effects of ESI Funding
Many studies have already looked at the potential effects of ESI funding. Above all they have found a positive influence on economic growth,73 benefiting rural areas, especially those near urban centres.74 This effect of ESI funding has subsisted after the most recent financial crisis75 and is also discernible in the most recent funding period, 2014 to 2020, albeit slightly weaker than previously.76 Some funded regions also show an improved medical infrastructure.77 Moreover, national authorities have occasionally used funding to take steps at the regional level to contain the Covid-19 pandemic.78
Alongside these positive findings, however, a series of studies also articulates doubts as to the comprehensive effectiveness of large-scale ESI funding. The focus is often on questions relating to the causal mechanism between funding and development79 and the quantification of success.80 While this paper cannot provide an extensive analysis of the effectiveness of ESI funding, previous research does show that several funded regions have experienced positive economic development. However, questions about precise causal relationships remain open. In line with these debates, the causal relationship between funding and the reduction of health inequalities also needs to be examined further since funding can have direct and indirect influences on public health and health care.
The direct influence of ESI funds runs via the funding of projects to improve health care in EU member states. According to previous contributions, ESI funds are suitable for reducing health inequalities by improving access to medical infrastructure and addressing health risks, especially those to which vulnerable groups are exposed.81 The funds were an important tool during EU enlargement, especially for new member states to overcome health care shortages and particularly where investment in the health system was a low priority in national budgets.82 For example, in Poland, a large part of the ERDF support was used for the expansion of hospitals.83 In Lithuania, health care reforms were comprehensively financially supported. While the ERDF directly addresses infrastructure, the employment-related ESF focuses primarily on the costs of training and only exceptionally on direct payments, for instance to recruit medical doctors in rural areas. However, the success of funding measures is often difficult to evaluate, as is general economic development after ESI funding, since no uniform metrics for measurement exist.
As well as these general projects, ESI funds were also specifically used to fight Covid-19, for example by co-funding the purchase of protective and respiratory equipment, especially in areas that had previously received little or no funding.84 Here, direct associations exist between the level of funding and the procurement of equipment and protective equipment. Furthermore, there were direct consequences for the population since existing facilities were improved and care capacities created. Studies also point to the relationship between investment in the health sector and the associated improvement of public health.85 Direct project funding can thus both top up member states (at times modest) health budgets and encourage further investment in a budget area that is often subject to cuts.86
When considering the effects of ESI funding on public health and health care, the level of funding must be placed into context with national health expenditure levels. According to the Cohesion Open Data Platform, around €389 m from the ERDF were used for Hungary’s health infrastructure during the funding period 2014 to 2020, for example. World Bank figures for 2019 put the country’s own health budget at around €10.3 bn. Similarly, Bulgaria received around €41 m from the ERDF during the same funding period, compared to its own budget of about €4.87 bn. Clearly, ESI funding only makes up a fraction of the total investment in the health sector; this is partly due to the fact that only 6.2 per cent of ESI funds were used for health in the funding period 2014 to 2020.
The share of funds invested in health projects is thus relatively low. However, ESI funding can also contribute to improving public health and health care indirectly, by stimulating general economic development.87
The Indirect Influence of ESI Funds
Because comparatively small ESI fund sums are used for health projects – and because of the economic determinants of health – much importance is attached to the indirect effects of ESI funds that concur with the regional economic development funding. A comprehensive study has shown that individual poverty and material deprivation only go so far in explaining differences in excess mortality during the pandemic. By contrast, the study showed that there was a positive association between lower regional economic development and excess mortality in the second year of the pandemic.88 This coincides with the findings of other studies whereby regional GDP is closely linked to indicators of objective and subjective health within the EU.89 In the EU, regional economic development thus seems to be especially significant in fighting health threats. Given the positive effects of ESI funding on regional economic growth, it can therefore be assumed that this funding also has an indirect effect on public health and health care – not least because the economic development of regions also goes hand in hand with building and expanding medical infrastructure. The causal mechanism here runs via the relationships between economic development and health spending90 and between health spending and the quality of health care (measured as the public’s satisfaction with the national health system).91
Further Funds to Enhance Health Care
There are other funds alongside the ESI funds that support health in the EU. The most important are “EU4Health”, “Horizon Europe”, “InvestEU” and the “Recovery and Resilience Facility” (RRF).
The EU regularly presents its new health programme EU4Health, which will run from 2021 to 2027, as a key element in building the EHU.92 This programme, the EU’s fourth on health, has a noticeably bigger budget than its predecessors, and is more ambitious too. The EU’s third health programme (the immediate predecessor of EU4Health) had a budget of €46 m and targeted improvements in the areas of health threats, determinants and information. The new EU4Health fund has a budget of €5.3 bn. This markedly higher budget can be exclusively attributed to the experiences made during the Covid-19 pandemic. Before the pandemic, there were even debates over whether to cut the EU health programme entirely and integrate it into other funding initiatives instead, such as the ESF.93 The aims of EU4Health are improving health, fighting cross-border threats to health, digitalisation, implementing the pharmaceutical strategy and strengthening health systems.94 It also strives to dovetail with funds such as the ESF and ERDF to improve access to health care and regional medical infrastructure.95
The Horizon Europe programme and its predecessor Horizon 2020 have primarily funded research with a view to the United Nations’ Sustainable Development Goals (SDG).96 They also attached importance to research into health. However, this research naturally does not lead to a direct improvement in public health or in access to health services.
In contrast, the InvestEU programme has above all funded long-term infrastructure, research and development as well as digitalisation, with a focus on small and medium enterprises; here too health topics are important.97 For instance, it has funded projects to develop new technologies in health care and diagnostics and made strategic investments in the pharmaceutical sector.98
Finally, the temporary “Recovery and Resilience Facility” (RRF) was established as part of the NextGenerationEU programme and endowed with a budget of €723.8 bn to support member states in overcoming the consequences of the pandemic and simultaneously make them more resilient to future crises.99 Just under half of its budget goes on funding that does not need to be repaid. Alongside the more general stimulation of economic growth, the RRF also encompasses projects that are directly related to health. These include, for instance, projects to enhance cooperation between EU member states of the health-care professions, patient organisations, the public administration of the health system and actors from education and academia,100 as well as projects to build centres to improve the prevention, diagnosis and treatment of cancer.101
These and other funds have more or less direct links to health topics. The ERDF and ESF, by contrast, are primarily intended for building and expanding medical infrastructure and contributing to the socio-economic convergence of regions. This raises the question of what role the ERDF and ESF can play in improving health within the EU and in building the EHU.
Improving Health in the EU
The EU always used the ESI funds as its primary instrument for contributing to the improvement of public health and population health care, especially until the new version of its health programme, EU4Health. The EU’s competencies in this area are distinctly limited by Articles 4, 6 and 168 TFEU.
Based on the above outlined health disparities in the EU and on the discussed literature on the effects of EU funds, this paper examines the hypothesis that ESI funds can improve regional medical infrastructure. In doing so, the research paper analyses whether ESI funds support the construction of resilient health systems and thus enable EU member states to confront future outbreaks of disease more effectively. This analysis requires a specific research design that makes it possible to determine the impact of funding on both medical infrastructure and resilience during the pandemic while controlling for other influencing factors.
Measuring the Effects of ESI Funds
A methodical challenge when measuring the effects of ESI funds is that, occasionally, projects can run for a long time. While some projects can be wrapped up in just a few years, certain bigger projects – for instance to expand or transform hospitals – may last up to five years or more. Moreover, the allocation of project funding is fixed for the respective multiannual financial framework (MFF), but the actual payout can also occur later. The most recent funding period before the pandemic, from 2014 to 2020, is therefore too recent to lend itself to measuring the effects in 2020 and 2021. This paper’s focus is thus on funding in the period 2007 to 2013.
It can be assumed that the majority of projects from the funding period 2007 to 2013 were completed by the first year of the pandemic in 2020. This makes it possible both to compare the changes in medical infrastructure in the funded regions between 2006 and 2020 and to examine whether the funded regions survived the pandemic better than others. Since ESI funding existed before 2007, it could be argued that the effect of previous funding periods should also be investigated. However, these funding rounds occurred before the EU’s Eastern enlargement or at best in its early days. As described above, the Eastern European regions were particularly hard hit by the pandemic. From a methodological perspective, it is therefore logical to foreground the ESI funding that benefited those regions. As a consequence, this research paper’s analysis of ESI funding focuses on the funding period 2007 to 2013.
Improving Medical Infrastructure
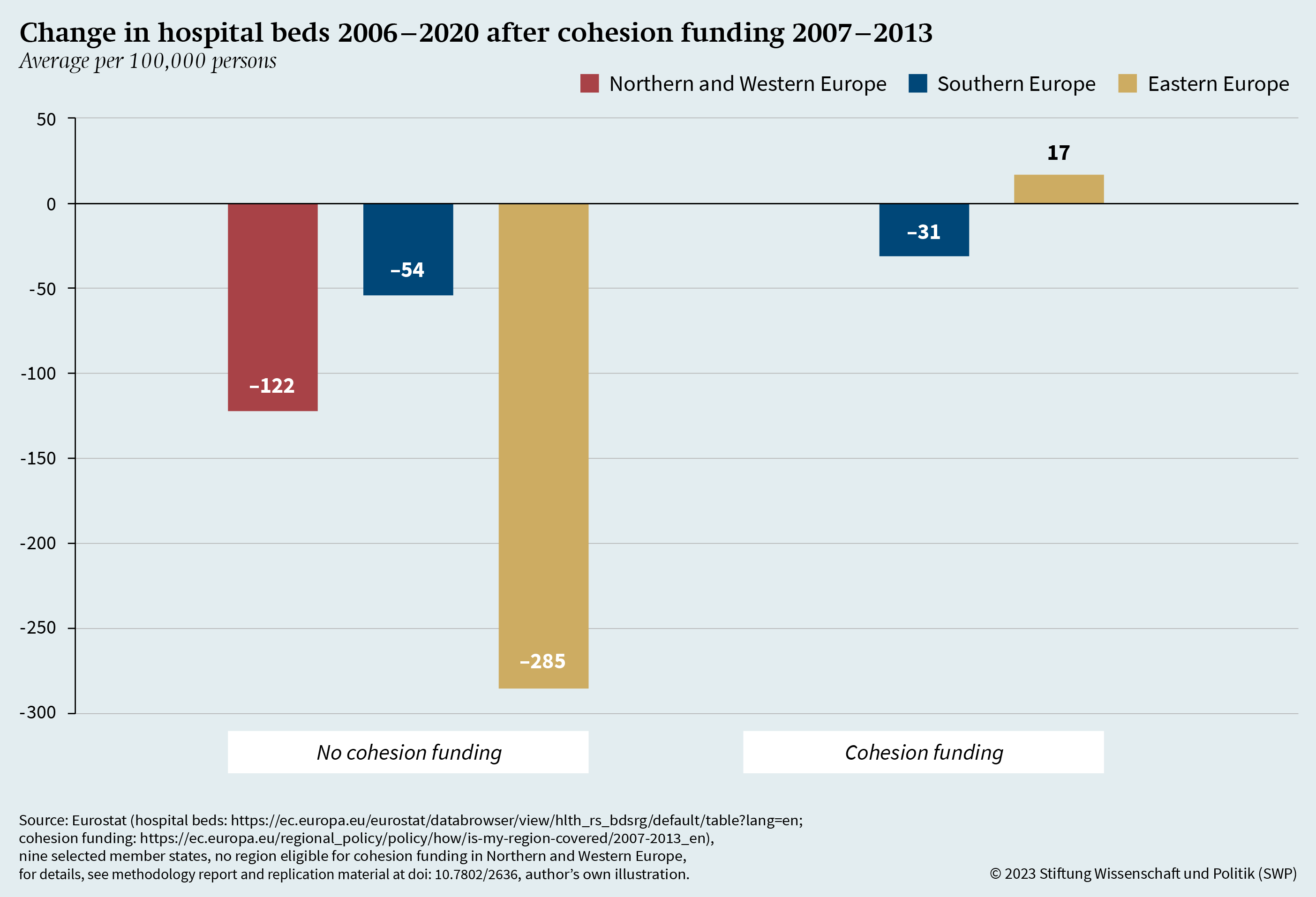
Based on previous research on the impact of ESI funding, the hypothesis is derived that funding improves medical infrastructure. To test this hypothesis, the paper analyses the changes in medical doctors and the number of hospital beds, in each case proportionately to population and from 2006 onwards, in other words before the 2007 funding. Figure 12 presents the changes in medical doctors since 2006 dependent on receiving extensive cohesion funding.102
The figure shows that, on average, all territorial units in the three EU regions have gained medical doctors since 2006. However, territorial units eligible for cohesion funding registered larger increases. This is particularly true for Eastern European NUTS regions eligible for cohesion funding. These 23 regions had far larger increases in medical doctors than the two Eastern European territorial units that were not eligible for cohesion funding. In the Southern Europe, the distribution is somewhat more balanced, with 16 funded and 29 non-funded regions. Additionally, the discernible difference is also smaller.
The overall positive increase in funded regions also represents a positive development in regional convergence (see Figure A.5). In 2006 the number of doctors in the eligible Eastern European territorial units still stood at 271 per 100,000 inhabitants and thus markedly below the two non-eligible Eastern European territorial units (527 per 100,000 inhabitants). Similarly, in the Southern EU member states, the eligible units had 314 doctors per 100,000 inhabitants in 2020, the non-eligible units 379 per 100,000 inhabitants. Thirteen years after cohesion funding began in 2007, there is thus a noticeable convergence in medical doctors numbers in regions eligible for cohesion funding.
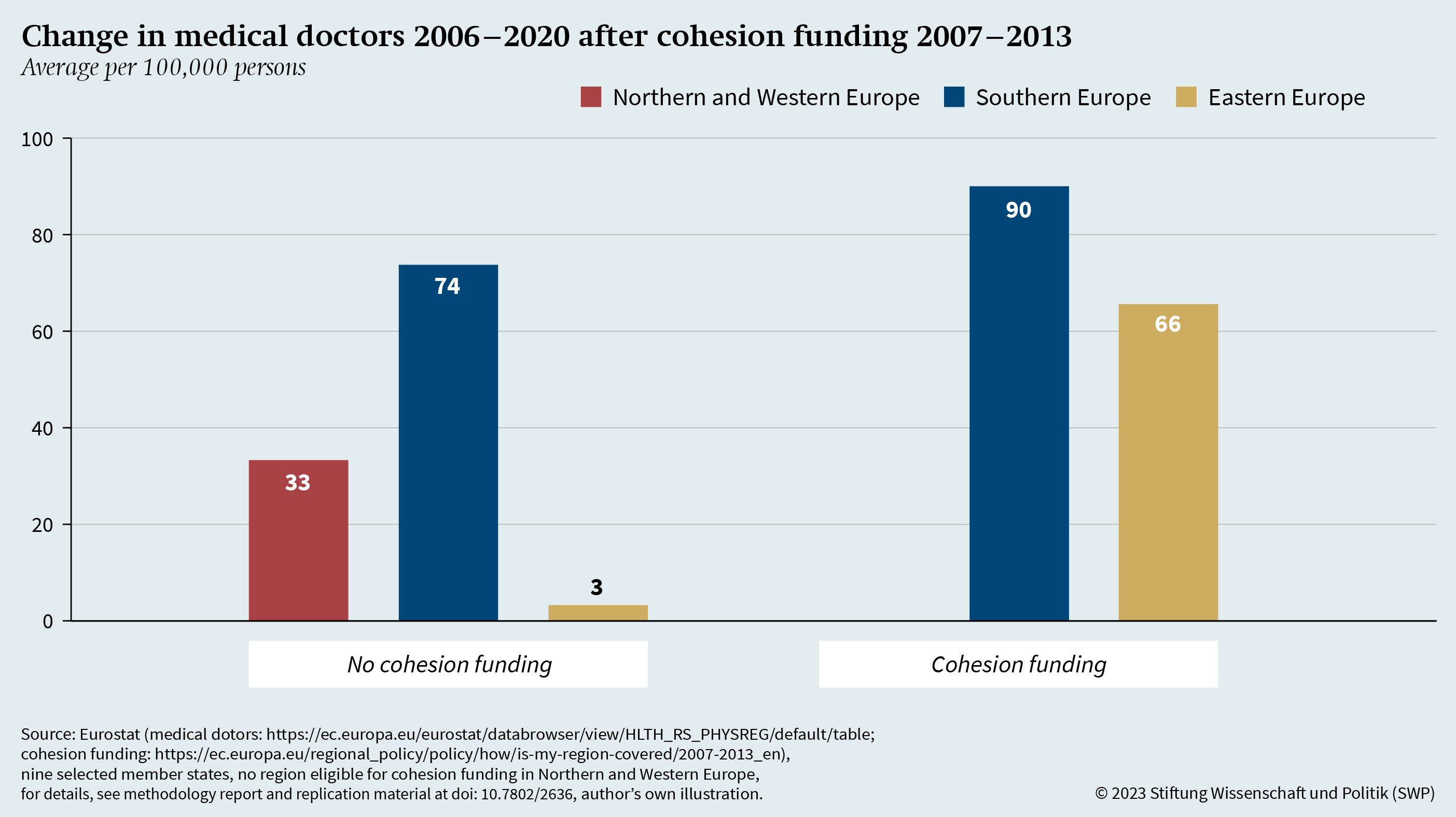
Figure 13 displays the average development in the number of hospital beds per 100,000 people in the analysed territorial units.103 Once again, the analysis distinguishes between areas that do and do not qualify for cohesion funding. Unlike with medical doctors, the number of hospital beds has dropped in almost all regions. Only the eligible Eastern European territorial units show a positive development.
What is particularly notable is the marked decrease in the number of hospital beds per 100,000 people in the two Eastern European territorial units without cohesion funding. In Southern EU member states, the funded areas registered a (minimally) less negative change in the number of hospital beds. As with medical doctors, numbers of hospital beds before funding started show that, on average, the non-eligible regions had more hospital beds than the eligible ones (see Figure A.6). In 2006 the number of hospital beds per 100,000 people was 399 in non-eligible Southern European territorial units but 335 in the regions funded after 2006. The difference very pronounced in territorial units in Eastern Europe. Non-funded units had an average of 935 hospital beds per 100,00 people in 2006. Funded units, by contrast, had only 670 hospital beds on average per 100,000 people before funding started. The positive development in the number of hospital beds in Eastern European areas during the cohesion funding periods is thus even more marked than with medical doctors.
Further calculations (see Tables A.2 und A.3) support these findings. They show that the positive change in the number of hospital beds in Eastern European areas particularly correlates with cohesion funding – when controlling for other potential factors and taking into account country-specific differences. According to the statistical models, however, the positive development in medical doctors is not significant across all regions. In this sense, it is particularly the positive development in the number of hospital beds that the analysis attributes to the effects of ESI funding.
Building Resilient Health Systems through ESI Funding
The third and last hypothesis states that ESI funding can support the building of resilient health systems. Here again the previously outlined challenges apply of working out the impact of cohesion funding. Research into the effects of funding normally uses more complex econometric models, which compare territorial units that have received cohesion funding with similar units that have not.104 The basic approach here is to scrutinise territorial units near the cut-off point of 75 per cent of the GDP pc pps for any differences.
|
Figure 13
|
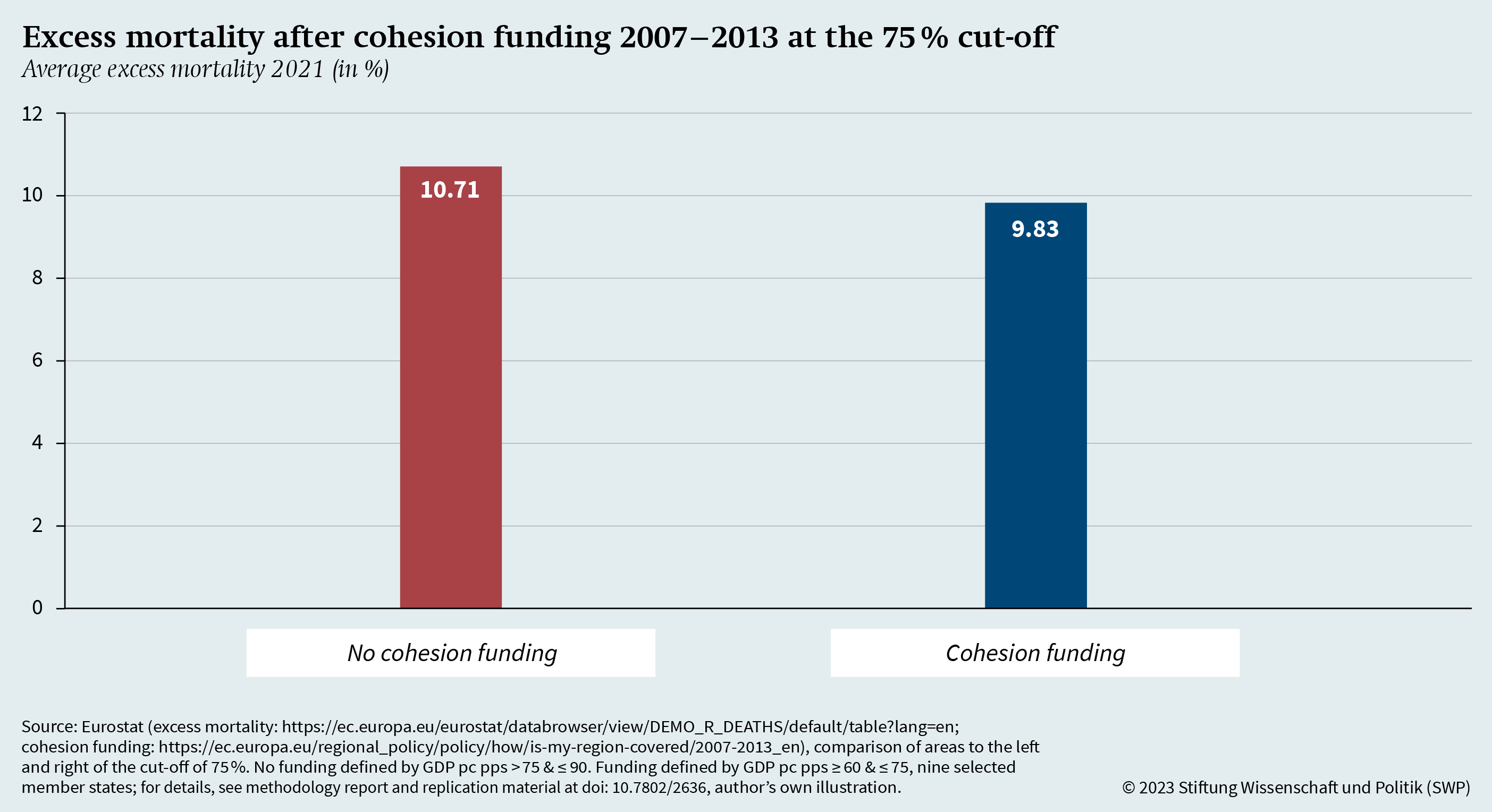
Using this approach, Figure 14 shows the excess mortality in regions that are 15 percentage points above and below the cut-off point. There are 11 territorial units in the 60 to 75 per cent range, and thus below the cut-off, which received cohesion funding between 2007 and 2013. The average excess mortality in these regions stands at 9.8 per cent. In the range 75 to 90 per cent of the EU’s GDP pc pps-average, there are 11 unfunded territorial units. In them, the average excess mortality in 2021 was 10.7 per cent, only 0.9 percentage points above the average of the funded regions.
The more complex analysis taking into account a number of other potential influences comes to the same conclusion. This analysis employed a regression discontinuity design to examine whether there is a “local average treatment effect” (LATE) due to cohesion funding at the cut-off point of 75 per cent (see Table A.4). This was not the case. It can thus be deduced that the areas which have received cohesion funding do not systematically differ from comparable units without cohesion funding in terms of excess mortality during the pandemic. However, as discussed above, the economic determinants of health are especially important. Hence, there is a possibility that territorial units which are still in the process of convergence do not yet show any effects because their economic cohesion is not yet complete, and they consequently have no greater resilience to health crises either. In analysing the potential influence of cohesion funding, the focus must thus be particularly on areas with successful funding.
Successful Funding of Regions
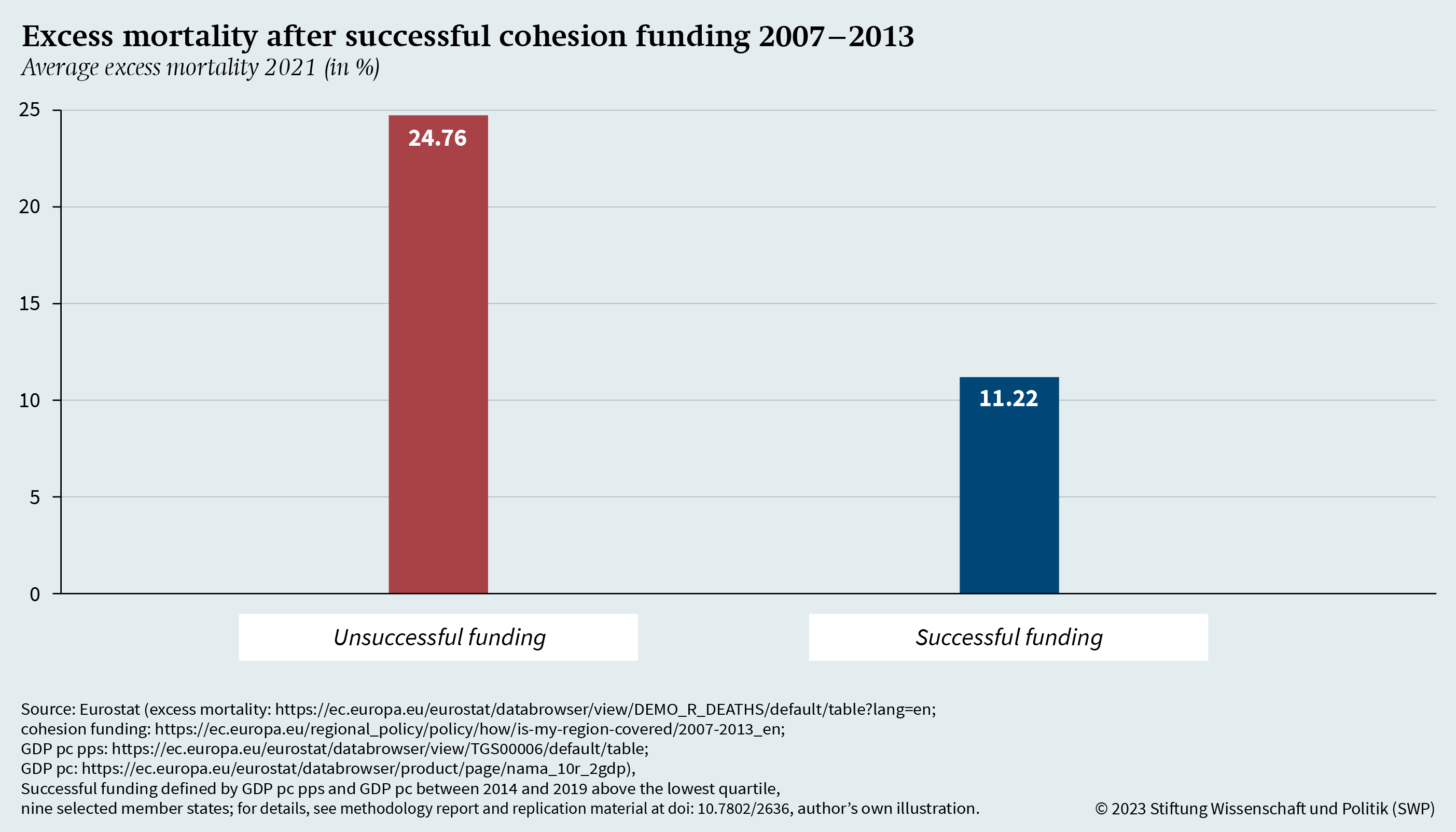
This research paper defines areas as successfully funded if they qualified for cohesion funding between 2007 and 2013 and belonged to the richest 75 per cent of the EU’s NUTS-2 regions, measured by its GDP pc pps and GDP pc between 2014 and 2019. By definition, unsuccessfully funded areas thus remain among the poorest 25 per cent of the EU’S NUTS-2 regions after funding. Under the differentiation employed here, there are 30 so far unsuccessfully funded areas versus nine successfully funded ones.
This finding might give rise to doubt over ESI funding and its use as a convergence instrument. However, the examined period of 2007 to 2013 was a funding period that strongly supported regions from new Eastern European member states; territorial units in Northern and Western Europe had already been successfully funded prior to 2007.105 The funding period 2007 to 2013 also fell into the Euro crisis, during which the effect of ESI funding has been shown to be positive still, though certainly weaker.106 The criterium for success is also based on the relative economic development of other areas. In other words, funding being unsuccessful does not automatically mean that there was no positive development in the GDP of a territorial unit but only that the relative GDP did not converge – be it due to slow growth in the territorial unit or faster growth in others. The results of the comparison are presented in Figure 15.
This figure shows a difference in the average excess mortality between already successfully funded and not yet successfully funded territorial units: in the 30 so far unsuccessfully funded areas the excess mortality in 2021 was 24.8 per cent on average while it was only about 11.2 per cent in the nine successfully funded areas. The positive correlation with successful funding also remains when other influencing factors are controlled for (see Table A.5). However, the distribution within the groups is also interesting. The nine successfully funded territorial units are in Italy (Basilicata), Portugal (Alentejo and Algarve), Spain (Galicia, Asturia, Castilla-La Mancha, Andalucia and Murcia) and Romania (Bucharest-Ilfov). While the successfully funded Southern European regions have an average excess mortality of 8.2 per cent, Bucharest-Ilfov is far above the average with 35.8 per cent, despite its positive economic development.
However, a few of the so far unsuccessfully funded areas had relatively low excess mortality. These include the Norte region (7.0 per cent) and the Azores (3.9 per cent) in Portugal, and Extremadura in Spain (8.1 per cent). Conspicuously, the unsuccessfully funded territorial units with low excess mortality are also located in Southern Europe. Despite the lower economic development of these units, their excess mortality is markedly lower than in the previously mentioned successfully funded territorial unit in Romania. While economic development – also triggered by ERDF and ESF funding – thus correlates with lower excess mortality, there are some rare divergences from this general trend. The next chapter will examine these divergences in detail.
Case Study of Selected Territorial Units
This explorative analysis is limited to territorial units with positive economic development and high excess mortality and to unsuccessfully funded territorial units with low excess mortality and a comparatively low GDP pc pps in per cent of the EU average. Bucharest-Ilfov (RO32) in Romania and Yugozapaden (BG41) in Bulgaria were chosen to represent areas with positive development. The latter does not fall into the category of successfully funded regions, analysed in the previous chapter, due to its GDP pc development; it nevertheless shows a positive economic development relative to the EU average. The unsuccessfully funded areas are represented by Norte in Portugal (PT11) and Extremadura in Spain (ES43).
The aim of the analysis is to identify systematic differences between these four territorial units to draw conclusions on the determinants of excess mortality that will have to be considered in building the EHU, alongside the already discussed medical infrastructure and economic determinants of health. Possible determinants can be grouped into four categories: Economic development, medical infrastructure, vulnerability of the population, and capacities for fighting pandemics (see Table 1).
The table shows that the selected areas differ noticeably in their economic development. While all units ranked below 75 per cent of the EU’s GDP pc pps average in the years 2000 to 2002 and were thus eligible for funding in the period 2007 to 2013, the areas in Portugal and Spain still fall short of the 75 per cent mark between 2014 and 2019. The opposite is true for the areas in Bulgaria and Romania. In Bulgaria’s Yugozapaden, the GDP pc pps rose from 39.3 per cent to 81.2 per cent, in Romania’s Bucharest even from 55.3 per cent to 142.7 per cent.
While there are substantial differences in the medical infrastructure between the regions, this cannot explain the variance in excess mortality since the so far unsuccessfully funded areas in Romania and Bulgaria largely have a better infrastructure than the other two regions. Their number of doctors, for instance, resembles that of areas with low excess mortality – in Bucharest-Ilfov it is even markedly higher. And the number of available hospital beds is twice or even three times as high in Yugozapaden and Bucharest-Ilfov as it is in the areas in Portugal and Spain.
Indicators of population vulnerability can likewise only provide a limited explanation for differences in excess mortality. The high population density in the Bucharest region carries the risk that a virus might spread quicker and wider; however, the Yugozapaden region also has high excess mortality despite having a population that is markedly less dense and comparable with that of the other selected regions. The population in the two Eastern European territorial units is also slightly younger and is, on average, significantly better educated than the populations in the Portuguese and Spanish regions. It can therefore not be assumed that the population in the Romanian and Bulgarian region has had a systematically increased vulnerability to the pandemic.
However, there are systematic differences in the indicators used to measure capacities for fighting pandemics. The number of tests carried out and the vaccination rate are substantially lower in the two Eastern European regions than in the two Southern European regions. On the one hand, the vaccination rate needs to be interpreted with caution due to the chronological differences in starting vaccination campaigns and due to the country-specific variance in vaccination scepticism.107 The differences in the number of tests carried out, on the other hand, are particularly revealing. In Portugal and Spain, every person on average was tested more than once; in Bulgaria and Romania only every second person was tested. These findings coincide with those of studies on excess mortality in Romania and Bulgaria. According to these studies, insufficient testing capacities and deficiencies in data transmission and in the associated identification and isolation of infected persons were among the contributing factors to excess mortality.108 Regardless of the chronological differences in starting vaccination campaigns, the lower vaccination rate in Romania and Bulgaria is also cited as a possible explanation for the higher excess mortality.109 However, the differences concern not only the specific capacities to fight pandemics: given the low investment in their health systems, Bulgaria and Romania also have low general capacities for fighting health threats.
|
|
|
|
|
|
|
Territorial units |
BG41 |
RO32 |
PT11 |
ES43 |
|
Economic development |
||||
|
Funding through ESIF 2007–2013 |
Yes |
Yes |
Yes |
Yes |
|
Average GDP pc pps 2000–2002 (% EU Avg.) |
39.3 |
55.3 |
63.3 |
58.7 |
|
Average GDP pc pps 2014–2019 (% EU Avg.) |
81.2 |
142.7 |
66.0 |
65.8 |
|
Medical infrastructure |
||||
|
Medical doctors (per 100,000 persons) |
468.4 |
656.3 |
561.0 |
370.4 |
|
Hospital beds (per 100,000 persons) |
757.6 |
1,028.0 |
342.2 |
349.8 |
|
Population vulnerability |
||||
|
Population density (per sq km) |
103.7 |
1,322.0 |
169.3 |
26.0 |
|
Population age (median) |
42.8 |
41.0 |
45.7 |
45.6 |
|
Education 2020 (higher secondary/tertiary in %) |
92.5 |
91.0 |
49.2 |
47.7 |
|
Capacities for fighting the pandemic |
||||
|
Covid-19 tests 2021 (per 1,000 persons) |
429.2 |
518.9 |
1,369.2 |
1,016.0 |
|
Positive test results (as % of all tests) |
8.6 |
8.5 |
4.5 |
8.5 |
|
Vaccination rate 2021 (as % having had at least the first dose) |
24.2 |
39.3 |
91.0 |
81.8 |
|
Health spending (in € per person) |
379.1 |
532.0 |
1,206.5 |
1,703.8 |
|
Measures 2021 (Oxford Response Tracker) |
48.4 |
62.3 |
60.2 |
55.4 |
|
Excess mortality 2020 (in %) |
14.9 |
16.6 |
17.4 |
15.4 |
|
Result |
||||
|
Excess mortality 2021 (in %) |
40.7 |
35.8 |
7.0 |
8.2 |
|
BG41: Yugozapaden (Bulgaria); RO32: Bucharest-Ilfov (Romania); PT11: Norte (Portugal); ES43: Extremadura (Spain) |
||||
In Bulgaria, measures to contain the pandemic were also noticeably less far-reaching on average compared to those in the other regions. This might be linked among other factors to the government of Boyko Borisov, which was in office until April 2021. Populist governments such as Borisov’s tendentially took less extensive measures and often spread disinformation on the pandemic.110 Alongside economic determinants of health and medical infrastructure, specific capacities and the willingness to fight health threats are thus also crucial. The low number of tests and the low investment can be cited as examples and proof.
The insight that capacity-building beyond the medical infrastructure is also crucial has fundamental implications for creating the EHU. The initiatives aimed at building the EHU currently focus on strengthening inter-state coordination in fighting cross-border health threats. Improving the resilience of health systems and health care in individual member states receives less attention.111 This is unsurprising since health care explicitly falls under the responsibility of member states.112 Nevertheless, the EU will have to address health care and capacity-building as well since deficiencies in the health care provision in individual member states weaken the EU overall in combatting threats. For the EHU not to fall short of its aspirations, the EU will have to push ahead with building available capacities, for instance by systematically identifying gaps and developing an integrated strategy for combining ESI funds with others funds, like EU4Health.
According to studies, another factor is highly relevant alongside the available capacities and the respective government’s measures: the trust that the population has in its government, which plays a part both in whether citizens follow public health recommendations and how people contribute to carry-out pharmaceutical and non-pharmaceutical interventions.113 While this paper does not examine trust in the government, trust was taken into consideration in the data analysis, as were the previously discussed determinants.
The case study provides an explorative analysis of the systematic differences between territorial units. The juxtaposition has shown that these differences only exist systematically for capacities to fight the pandemic, not in the areas’ general medical infrastructure or economic profile. In the interest of building the EHU, the EU must therefore not only strengthen the regions through ESI funding and the expansion of medical infrastructure, but it also needs to systematically support the individual member state’s regional capacities in primary health care, especially in prevention and diagnosis.
Summary and Conclusions
The pandemic has affected EU member states to varying degrees. Subnational disparities have come to light, which are reflected in the great variance of excess mortality rates at the regional level. Based on these differences, the determinants for the lack of resilience of national healthcare systems can be identified and paths for improving healthcare provision within the EU can be pointed out. A special focus of this paper was the evaluation of ESI funding as a means of building the EHU. This focus derives on the one hand from the political relevance of these funds. The European Commission is currently preparing its evaluation of the multiannual financial framework, and it is already becoming apparent that ESI funds will be considered less and less as means to promote cohesion and convergence and more as means to strengthen already prosperous regions. On the other hand, EU funds in particular are capable of influencing the socio-economic determinants of health, which are closely linked to the economic development of individual regions.
This paper has addressed two research questions: How can regional differences in excess mortality during the Covid-19 pandemic be explained; and how can public health disparities be overcome within the framework of EU governance? Based on previous research, three possible answers were posited to guide the analysis: economic deprivation as well as the condition and quality of medical infrastructure influence excess mortality; ESI funding leads to an improvement in medical infrastructure; ESI funding supports resilience-building in health care systems.
To begin with, this paper devised a cartography of the Covid-19 pandemic. The European Commission has already suggested in its analyses of the pandemic that differences in excess mortality are linked to differences between urban centres and rural areas.114 However, this study found that it is less rurality per se than the economic profile of individual regions which explains differences in excess mortality. The research paper has shown that the pandemic started in urban, economically well-developed regions in spring 2020 before spreading into rural and economically rather disadvantaged regions in the second half of 2020 and especially in 2021.
The paper’s focus on economically less developed regions lead to the discovery that the pandemic has reinforced existing health disparities within the EU. For example, life expectancy in the economically less developed Eastern European regions diverges sharply from life expectancy in the other EU regions – as it did before the pandemic. The fact that other indicators, such as infant mortality, have largely fallen in line with other regions should be seen as an exception. However, the disparities show not only in the indicators that shed light on the state of public health but also in differences in medical infrastructure between individual regions, even though these are less clearer than expected.
Regarding the link between medical infrastructure, economic development and excess mortality, this analysis concluded that the proportion of doctors, unlike the density of hospital beds, does not correlate with excess mortality. Controlling for other influencing factors showed that medical infrastructure in the form of hospital beds is associated with regional excess mortality. However, the correlation between excess mortality and economic development was even more pronounced. Across almost all the territorial units, higher excess mortality in the pandemic’s second year was associated with a lower GDP pc. Here too other influencing factors were controlled for. The analysis further took into account that economically better developed areas in particular experienced excess mortality in the pandemic’s first year because of their greater exposure, resulting in greater resilience at later stages of the pandemic.
After identifying the relevant economic determinants of health during the pandemic, the question arose how these could be influenced with a view to making EU health care more resilient and building the EHU. The research paper therefore examined the effects of ESI funding on medical infrastructure and the creation of more resilient public health. Previous research has already highlighted that ESI funding can have a positive effect on economic development and infrastructure. This leads to the question of whether the ESI funds will have a part to play alongside more specific health promotion programmes, such as EU4Health, in building the EHU.
The analysis shows that in funded territorial units the number of hospital beds in particular increases more than in unfunded areas. This is especially true for the economically deprived areas in Eastern European member states. This suggests that the positive development in hospital bed numbers especially translates into reduced excess mortality and greater resilience of the health system. The finding supports the hypothesis derived from the literature that ESI funding should be expected to have a positive influence on medical infrastructure. However, this positive influence is not only due to direct funding, such as the construction or expansion of hospitals, but also to the general economic development, which increases regional prosperity and thus attracts people, provides more medical doctors and makes investment in infrastructure possible or more attractive.
The third and final hypothesis to be analysed was therefore whether ESI funding was also reflected in greater resilience to health threats. For this, different territorial units during the Covid-19 pandemic were compared. The key indicator for resilience was once again excess mortality in the pandemic’s second year. The comparison showed that funded areas did not significantly differ from those without cohesion funding. This suggests that the funding per se had no direct effect on resilience during the pandemic. However, differences emerged when comparing successfully funded areas with unsuccessfully funded ones. The previously demonstrated correlation, whereby areas with greater economic power came through the pandemic better than those with smaller economic capacities, applied here too. In other words, while ESI funding per se does not correlate with lower excess mortality, successfully funded areas on average do present markedly lower excess mortality.
However, not all successfully funded areas register lower excess mortality. The case study juxtaposed two areas that had been especially hard hit in terms of excess mortality despite showing positive economic development with two regions which have not been successfully funded to date, but which nevertheless registered a low excess mortality. Despite their good economic development, the hard-hit areas differed most from the other areas in their capacity to react to the pandemic and in their investment in health.
Based on the analyses, this paper concludes that the differences in excess mortality, which can be observed between individual EU member states and particularly within EU countries, can be partly explained by the economic deprivation of individual regions. While medical infrastructure in the form of available hospital beds also plays a role, the correlation is clearest with economic determinants. Based on the literature and empirical analyses, this paper also shows that areas which have received cohesion funding from ESI funds registered a rise in the number of hospital beds. This is especially true for funded areas in Eastern EU member states. It would be logical if the increase in available hospital beds in funded regions in turn contributed to reducing excess mortality. However, the funding and improvement of infrastructure is not sufficient in itself to boost the resilience of individual areas to health threats. Rather, the analysis shows that funding must be followed by economic development and that specific capacities and material for countering health threats are also required. Where these are not available, areas register higher excess mortality despite their economic development and existing medical infrastructure.
Specific recommendations for action for German and EU policy and for health governance arise from the results of this research paper:
-
The ESI funds are highly important in building the EHU and creating a higher degree of resilience within EU health systems. The funds are the only instrument that creates economic cohesion and convergence between regions, and thus equivalent living conditions within the EU. They should especially be used as cohesion instruments for public health and health care because economic development is directly linked to population resilience to health threats. The ESI funds will thus complement other funds, such as EU4Health, in building the EHU and preparing for future outbreaks of disease. ESI funds should therefore be used in combination with other funds to strengthen population resilience and build robust health systems.
-
The cartography of the pandemic shows that a sole focus on rurality only carries limited power to explain differences in the regional excess mortality. Rather, in the EU, differences in excess mortality are systematically associated with economic deprivation. It must hence first be acknowledged that economic determinants of health play a decisive role in resilience to health threats even within the EU. Medical infrastructure in the form of available hospital beds also has some significance for resilience but this paper’s results clearly reflect the more robust correlation between economic development and excess mortality. To prepare for future health emergencies, the focus should therefore especially be on economically weak areas, which should be given the necessary capacities to fight the diseases outbreaks.
-
One possibility for better preparing areas for epidemics and pandemics is to work towards their economic convergence. Here, cohesion funding via the ESI funds can be used to create equivalent living conditions within the EU. This requires not only specific projects to enhance medical infrastructure but also general economic development, which will in turn have a positive effect on medical infrastructure and population health.
-
Alongside ESI funding, capacities for fighting acute dangers to health should be expanded and medical products, tests and protective equipment should be distributed quickly and fairly within the EU. Neither improved medical infrastructure in the regions nor economic development can compensate in and by themselves for a lack of materials to fight health threats.
-
A combination of various instruments will be indispensable to build the EHU and prepare for future epidemics and pandemics. The ESI funds are one of these instruments, which can bring about convergence and positively influence the socio-economic determinants of health. Building medical infrastructure has an important if secondary role. However, the EU must be enabled to react to health emergencies so robustly that the supply of medical and non-medical counter-measures to EU member states is guaranteed. This point in particular lends itself to a dovetailing of the ESI funds with the EU4Health programme.
Appendix
This appendix gives details on the results of the regression analyses discussed in the text and contains the descriptive figures referenced in the text. Each of the regression analyses presented in Tables A.1 to A.5 lists, in its left column, the independent variables included in the models. The arrows show the direction and the statistical significance of the correlation between the independent variables and the dependent variable in the respective model.
The replication materials and the methodological report can be found at doi: 10.7802/2636.
Tables
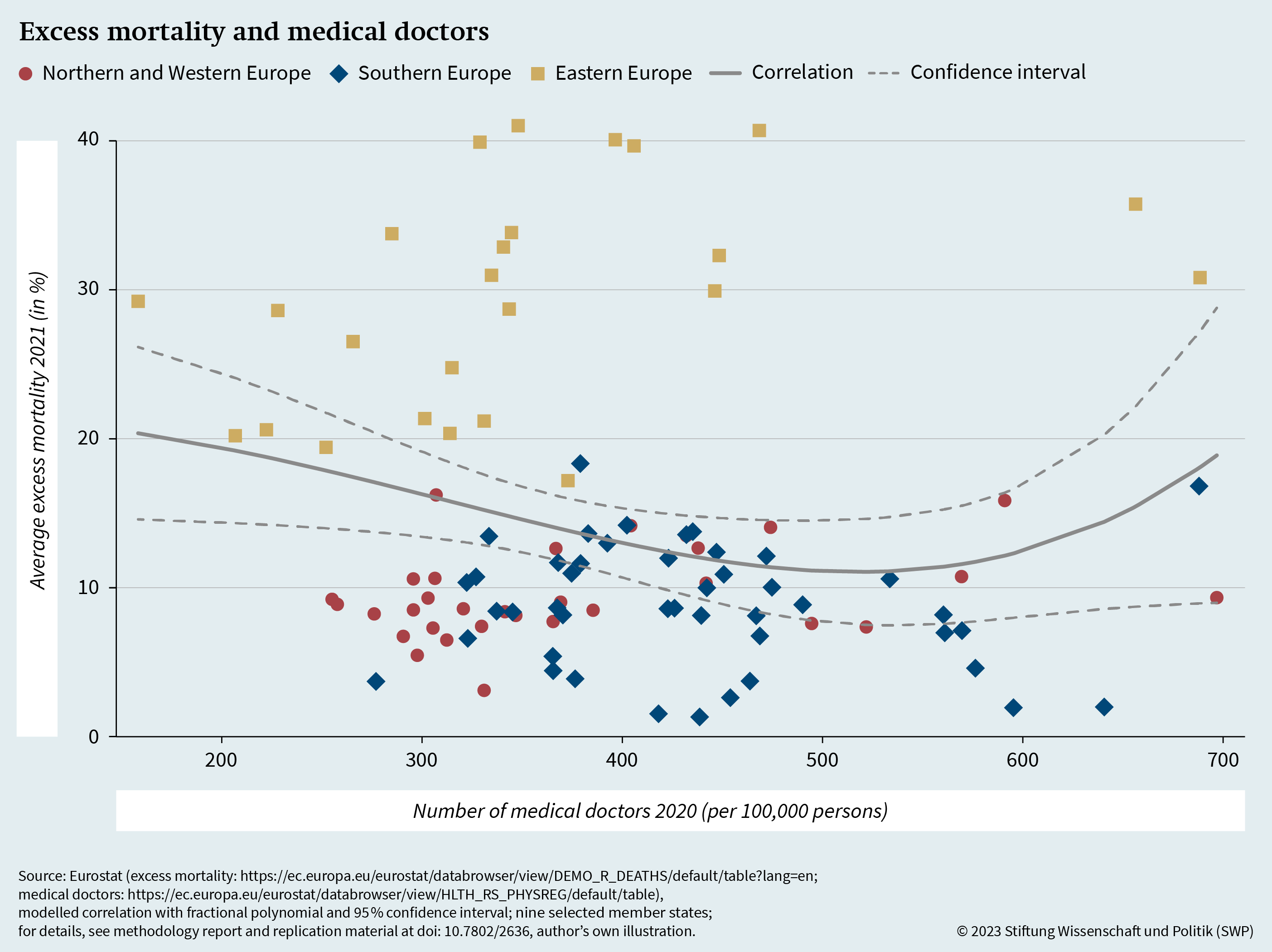
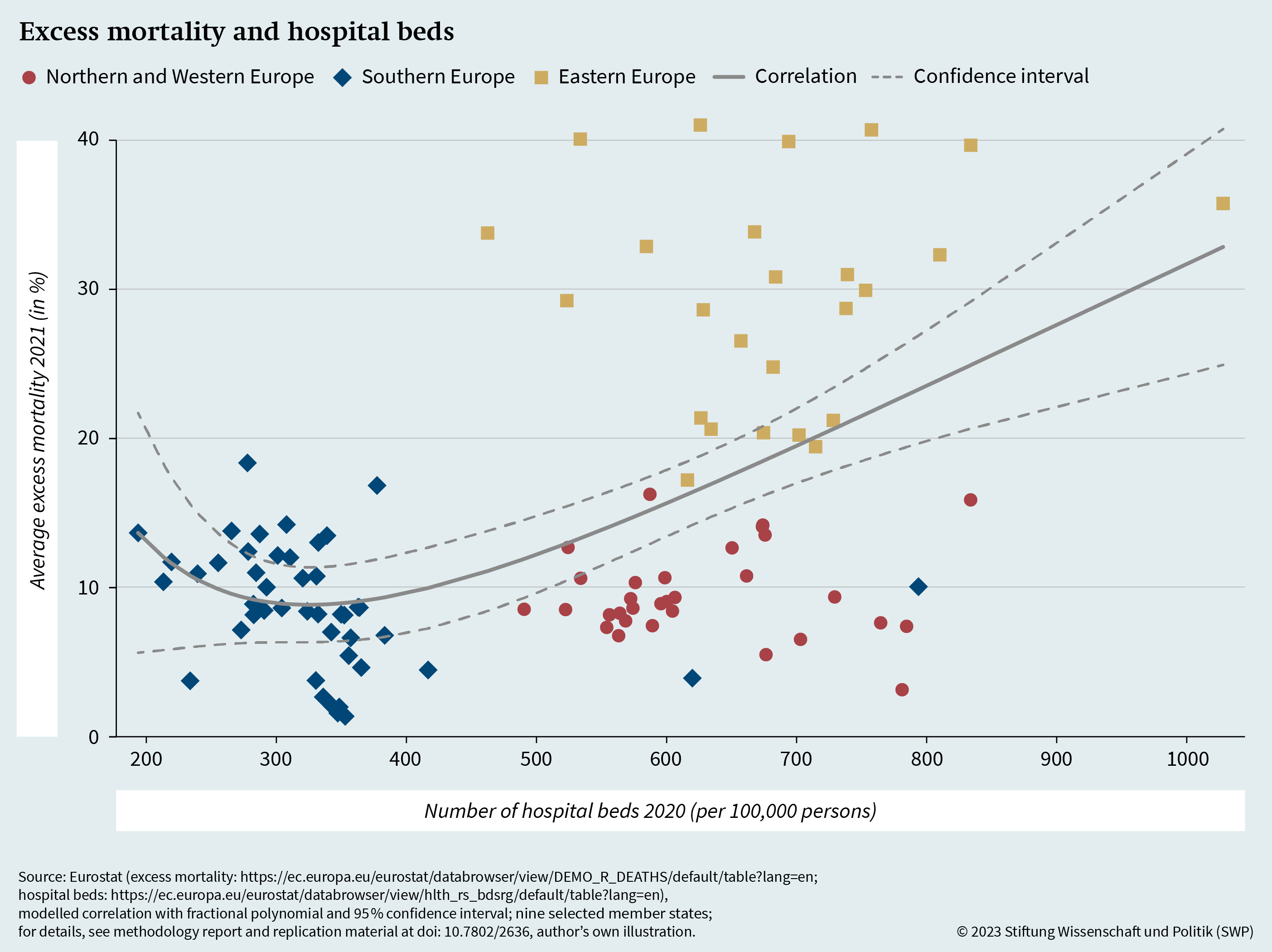
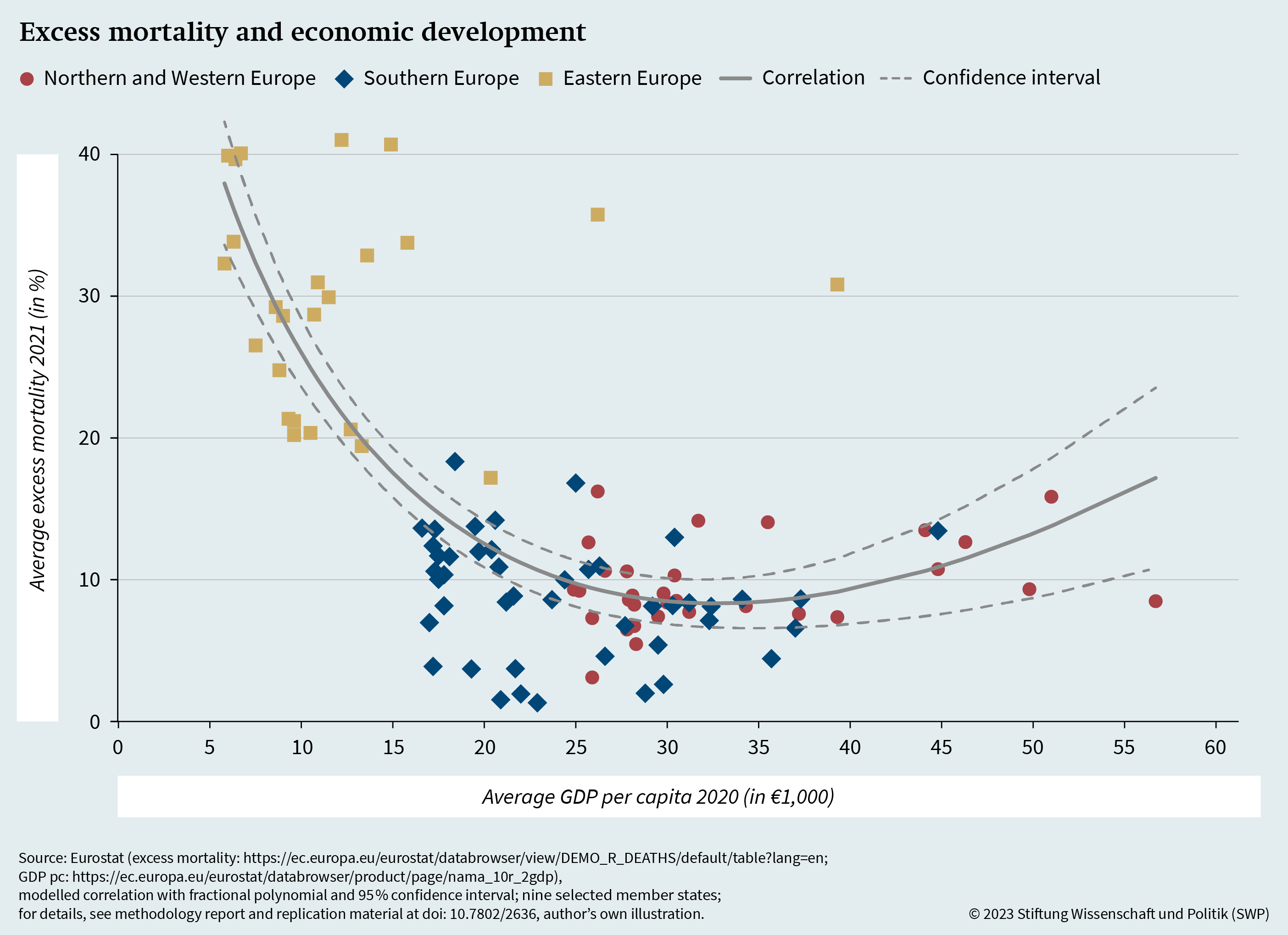
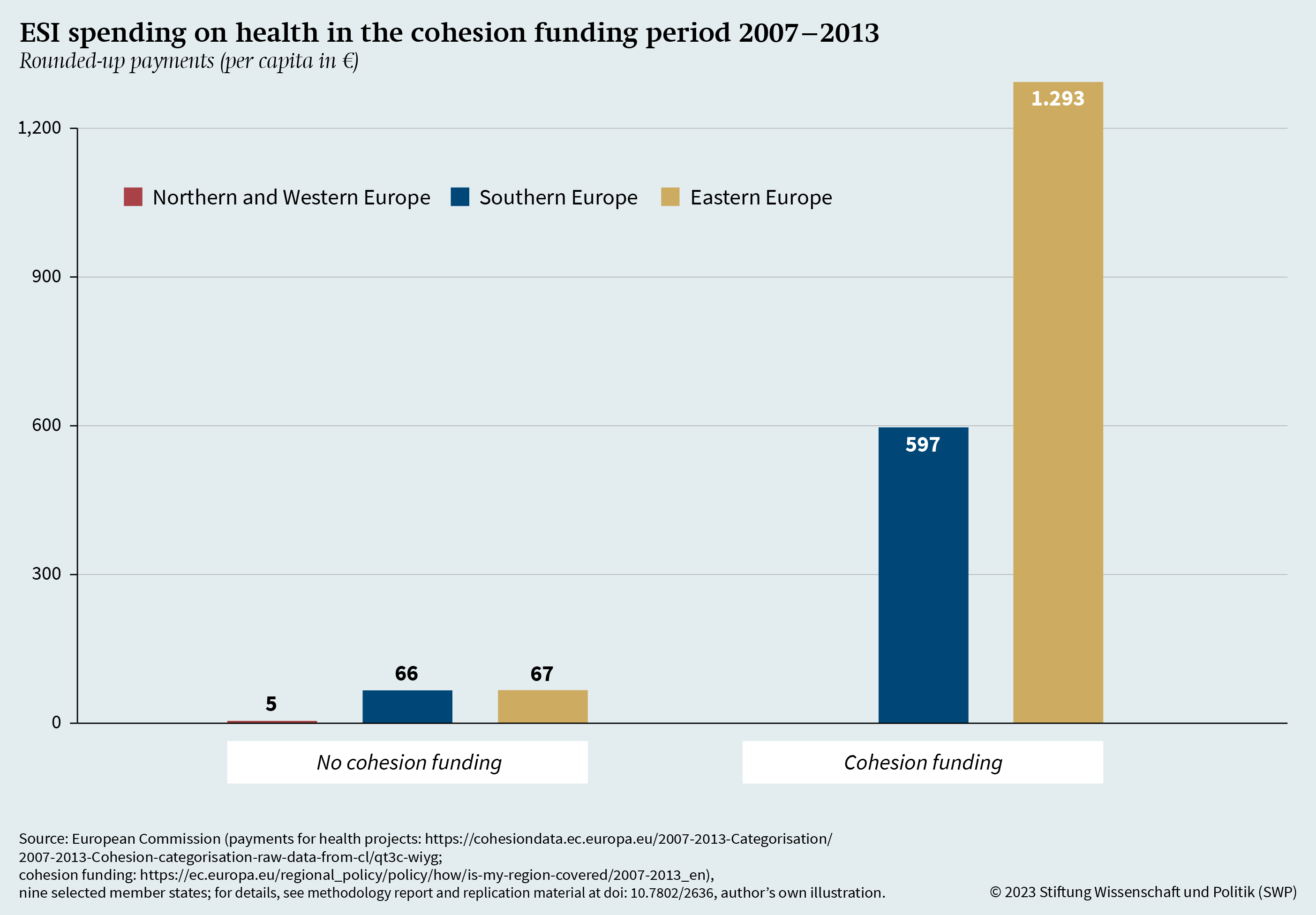
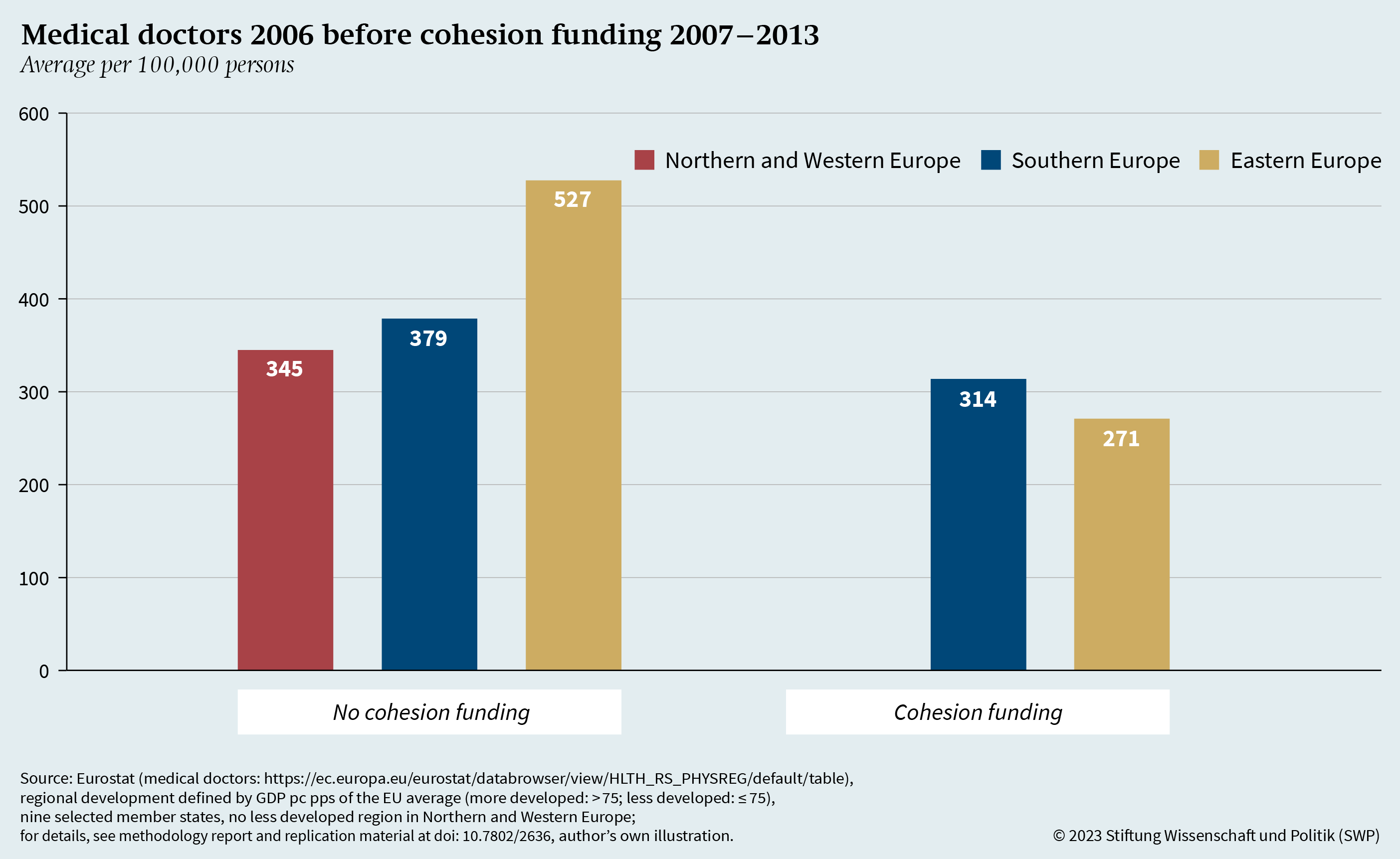
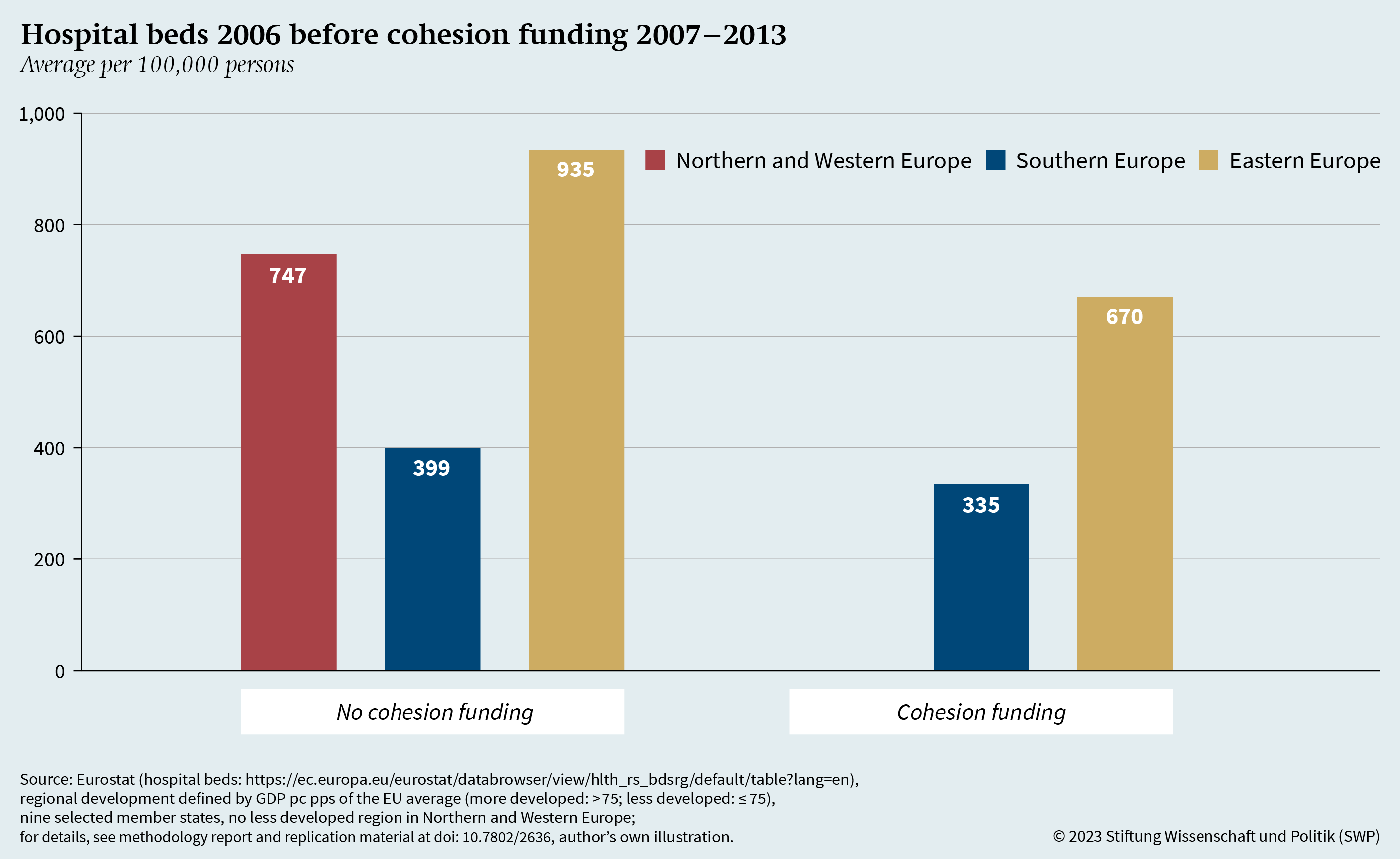
Abbreviations
|
BMG |
Bundesministerium für Gesundheit (Federal Ministry of Health) |
|
CF |
cohesion fund |
|
EAFRD |
European Agricultural Fund for Rural Development |
|
EFRD |
European Fund for Regional Development |
|
EHU |
European Health Union |
|
EMFAF |
European Maritime, Fisheries and Aquaculture Fund |
|
ESF |
European Social Fund |
|
ESI funds |
European Structural and Investment funds |
|
EU |
European Union |
|
GDP |
gross domestic product |
|
LATE |
local average treatment effect |
|
MFF |
Multiannual financial framework |
|
NUTS |
Nomenclature of statistical territorial units (from Fr. Nomenclature des unités territoriales statistiques) |
|
pc |
per capita |
|
pps |
purchasing power standard |
|
RRF |
Recovery and Resilience Facility |
|
SDG |
Sustainable Development Goals |
|
TFEU |
Treaty on the Functioning of the European Union |
|
WHO |
World Health Organization |
Endnotes
- 1
-
Fritz W. Scharpf, “The European Social Model”, Journal of Common Market Studies 40, no. 4 (2002): 645–70.
- 2
-
Scott L. Greer et al., Everything You Always Wanted to Know about European Union Health Policy But Were Afraid to Ask, 3rd ed. (Copenhagen: World Health Organization [WHO], 2022).
- 3
-
Anniek de Ruijter, EU Health Law & Policy. The Expansion of EU Power in Public Health and Health Care (Oxford: Oxford University Press, 2019).
- 4
-
European Commission, “Building a European Health Union: Stronger Crisis Preparedness and Response for Europe”, press release, Brussels, 11 November 2020, https://ec.europa. eu/commission/presscorner/detail/en/ip_20_2041 (accessed 25 July 2023).
- 5
-
European Commission, “European Health Union. Protecting Our Health Together”, https://commission.europa. eu/strategy-and-policy/priorities-2019-2024/promoting-our-european-way-life/european-health-union_en (accessed 25 July 2023).
- 6
-
Eleanor Brooks et al., “EU Health Policy in the Aftermath of COVID-19: Neofunctionalism and Crisis-driven Integration”, Journal of European Public Policy 30, no. 4 (2023): 721–39.
- 7
-
European Commission, “The Regional Impact of COVID-19”, March 2022, https://cohesiondata.ec.europa.eu/stories/s/ The-regional-impact-of-COVID-19/24gj-n8r2 (accessed 17 May 2023); Eurostat, “Excess Mortality – Statistics”, https://ec. europa.eu/eurostat/statistics-explained/index.php?title= Excess_mortality_-_statistics (accessed 17 May 2023).
- 8
-
World Health Organization (WHO), “Global Excess Deaths Associated with COVID-19 (Modelled Estimates)”, Geneva, 19 May 2023, https://www.who.int/data/sets/global-excess-deaths-associated-with-covid-19-modelled-estimates (accessed 21 December 2023).
- 9
-
Francesco Checchi and Les Roberts, Interpreting and Using Mortality Data in Humanitarian Emergencies, Network Paper (London: Humanitarian Practice Network, September 2005), https://odihpn.org/wp-content/uploads/2005/09/network paper052.pdf (accessed 25 July 2023); Michael Bayerlein et al., “Populism and Covid-19: How Populist Governments (Mis)handle the Pandemic”, Journal of Political Institutions and Political Economy 2, no. 3 (2021): 389–428.
- 10
-
Haldong Wang et al., “Estimating Excess Mortality Due to the Covid-19 Pandemic: A Systematic Analysis of Covid-19-related Mortality, 2020–21”, The Lancet 399, no. 10334 (2022): 1513–36.
- 11
-
Akash P. Kansagra et al., “Collateral Effect of Covid-19 on Stroke Evaluation in the United States”, New England Journal of Medicine 383, no. 4 (2022): 400–01; Mike Richards et al., “The Impact of the Covid-19 Pandemic on Cancer Care”, Nature Cancer 1, no. 6 (2020): 565–67; Matthew D. Solomon et al., “The Covid-19 Pandemic and the Incidence of Acute Myocardial Infarction”, New England Journal of Medicine 383, no. 7 (2020): 691–93.
- 12
-
Thomas Beaney et al., “Excess Mortality: The Gold Standard in Measuring the Impact of Covid-19 Worldwide?” Journal of the Royal Society of Medicine 113, no. 9 (2020): 329–34.
- 13
-
Garyfallos Konstantinoudis et al., “Regional Excess Mortality during the 2020 Covid-19 Pandemic in Five European Countries”, Nature Communications, 13 (2022) 1, article no. 482.
- 14
-
European Commission, “The Regional Impact of COVID-19” (see note 7).
- 15
-
The EU member states belong to the regions as follows. Northern and Western Europe: Austria, Belgium, Denmark, Finland, France, Germany, Ireland, Luxembourg, the Netherlands and Sweden; Southern Europe: Cyprus, Greece, Italy, Malta, Portugal and Spain; Eastern Europe: Bulgaria, Croatia, the Czech Republic, Estonia, Hungary, Latvia, Lithuania, Poland, Romania, Slovakia and Slovenia.
- 16
-
NUTS (from the French Nomenclature des unités territoriales statistiques) is the EU-wide uniform nomenclature for identifying territorial units. NUTS-3 corresponds to small regions (Landkreise in Germany), NUTS-2 to basic regions (Regierungsbezirke in Germany). The EU’s typology for rurality is based on population density per square kilometre, so-called grid cells. Urban areas are NUTS-3 regions in which over 80 per cent of the population live in grid cells of more than 300 inhabitants and where more than 5,000 people are registered. In intermediate regions only 50 to 80 per cent live in such urban grid cells; in rural regions, under 50 per cent.
- 17
-
Diego F. Cuadros et al., “Dynamics of the COVID-19 Epidemic in Urban and Rural Areas in the United States”, Annals of Epidemiology 59 (2021): 16–20; Robin Muegge et al., “National Lockdowns in England: The Same Restrictions for All, But Do the Impacts on COVID-19 Mortality Risks Vary Geographically?”, Spatial and Spatio-temporal Epidemiology 44, article no. 100559 (2023); Rajib Paul et al., “The Association of Social Determinants of Health with Covid-19 Mortality in Rural and Urban Counties”, The Journal of Rural Health 37, no. 2 (2021): 278–86.
- 18
-
Eurostat, “Excess Mortality – Statistics” (see note 7).
- 19
-
Giovanni Corona et al., “Diabetes Is Most Important Cause for Mortality in Covid-19 Hospitalized Patients: Systematic Review and Meta-analysis”, Reviews in Endocrine and Metabolic Disorders 22 (2021): 275–96; Xiaoyu Fang et al., “Epidemiological, Comorbidity Factors with Severity and Prognosis of COVID-19: A Systematic Review and Meta-analysis”, Aging (Albany NY) 12, no. 13 (2020): 12493–503; Adekunle Sanyaolu et al., “Comorbidity and Its Impact on Patients with Covid-19”, SN comprehensive clinical medicine 2, no. 8 (2020): 1069–76; Saskia Trump et al., “Hypertension Delays Viral Clearance and Exacerbates Airway Hyperinflammation in Patients with COVID-19”, Nature Biotechnology 39, no. 6 (2020): 705–16.
- 20
-
Paul Brandily et al., “A Poorly Understood Disease? The Unequal Distribution of Excess Mortality Due to Covid-19 across French Municipalities”, European Economic Review 140, article no. 103923 (2021); Hugo Pilkington et al., “Spatial Determinants of Excess All-cause Mortality during the First Wave of the Covid-19 Epidemic in France”, BMC Public Health 21, no. 1, article no. 2157 (2021).
- 21
-
Neftali E. Antonio-Villa et al., “Comprehensive Evaluation of the Impact of Sociodemographic Inequalities on Adverse Outcomes and Excess Mortality during the Coronavirus Disease 2019 (COVID-19) Pandemic in Mexico City”, Clinical Infectious Diseases 74, no. 5 (2022): 785–92.
- 22
-
Tania Alfaro et al., “Excess Mortality During the COVID-19 Pandemic in Cities of Chile: Magnitude, Inequalities, and Urban Determinants”, Journal of Urban Health 99, no. 5 (2022): 922–35.
- 23
-
Chiara Burlina and Andrés Rodríguez-Pose, “Inequality, Poverty, Deprivation and the Uneven Spread of COVID-19 in Europe”, Regional Studies, 15 March 2023, doi: 10.1080/ 00343404.2023.2172390.
- 24
-
“Regulation (EU) No 1301/2013 of the European Parliament and of the Council of 17 December 2013 on the European Regional Development Fund and on Specific Provisions Concerning the Investment for Growth and Jobs Goal and Repealing Regulation (EC) No 1080/2006”, Official Journal of the European Union, 20 December 2013, https://eur-lex. europa.eu/legal-content/EN/TXT/?uri=celex%3A32013R1301 (accessed 25 July 2023).
- 25
-
Burlina and Rodríguez-Pose, “Inequality, Poverty, Deprivation and the Uneven Spread of COVID-19 in Europe” (see note 23).
- 26
-
Johan P. Mackenbach, Health Inequalities: Europe in Profile, Report (Rotterdam, February 2006), http://envejecimiento. csic.es/documentos/documentos/ue-healthinequalities-01.pdf (accessed 25 July 2023); Anton E. Kunst et al., “Occupational Class and Cause Specific Mortality in Middle Aged Men in 11 European Countries: Comparison of Population Based Studies. Commentary: Unequal Inequalities across Europe”, BMJ 316, no. 7145 (1998): 1636–42; Annette Leclerc et al., “Differential Mortality: Some Comparisons between England and Wales, Finland and France, Based on Inequality Measures”, International Journal of Epidemiology 19, no. 4 (1990): 1001–10.
- 27
-
Johan P. Mackenbach et al., “Widening Socioeconomic Inequalities in Mortality in Six Western European Countries”, International Journal of Epidemiology 32, no. 5 (2003): 830–37.
- 28
-
Elizabeth A. Richardson et al., “Have Regional Inequalities in Life Expectancy Widened within the European Union between 1991 and 2008?” The European Journal of Public Health 24, no. 3 (2014): 357–63.
- 29
-
Johan P. Mackenbach et al., “The Unequal Health of Europeans: Successes and Failures of Policies”, The Lancet 381, no. 9872 (2013): 1125–34.
- 30
-
Vladimir M. Shkolnikov et al., “Educational Level and Adult Mortality in Russia: An Analysis of Routine Data 1979 to 1994”, Social Science & Medicine 47, no. 3 (1998): 357–69; Imre Boncz and Andor Sebestyén, “Economy and Mortality in Eastern and Western Europe between 1945 and 1990: The Largest Medical Trial of History”, International Journal of Epidemiology 35, no. 3 (2006): 796–97.
- 31
-
Zoltán Egri, “Regional Health Inequalities in the European Macroregion from the East Central European Perspective”, Regional Statistics 7, no. 1 (2017): 197–224.
- 32
-
WHO, Review of Social Determinants and the Health Divide in the WHO European Region: Final Report WHO Regional Office for Europe (Copenhagen, 20 May 2013, updated reprint 2014 [report]), https://www.who.int/publications/i/item/ 9789289000307 (accessed 25 July 2023).
- 33
-
Steven L. Gortmaker and Paul H. Wise, “The First Injustice: Socioeconomic Disparities, Health Services Technology, and Infant Mortality”, Annual Review of Sociology 23, no. 1 (1997): 147–70; Luc Onambele et al., “Infant Mortality in the European Union: A Time Trend Analysis of the 1994–2015 Period”, Anales de Pediatría (English edition) 91, no. 4 (2019): 219–27.
- 34
-
Eleanor Brooks, “European Union Health Policy after the Pandemic: An Opportunity to Tackle Health Inequalities?”, Journal of Contemporary European Research 18, no. 1 (2022): 67–77.
- 35
-
Enrico Ivaldi et al., “Objective and Subjective Health: An Analysis of Inequality for the European Union”, Social Indicators Research 138 (2018): 1279–95; Viktor Pál et al., “Concentration and Inequality in the Geographic Distribution of Physicians in the European Union, 2006–2018”, Regional Statistics 11, no. 3 (2021): 3–28; European Commission, “Inequalities in Access to Healthcare. A Study of National Policies 2018”, http://lekuvam.se/wp-content/ uploads/2020/03/26.-Baetenetal.ESPNInequalitiesinaccess tohealthcare.pdf (accessed 28 June 2023).
- 36
-
Analysis of 101 NUTS-2 regions in nine EU member states. For details, see the chapter on “Determinants of Covid-19 excess mortality in the EU” (pp. 20ff).
- 37
-
No region in the north-western EU is currently classified as “less developed” since none has a GDP pc pps of under 75 per cent of the average EU GDP.
- 38
-
Pál et al., “Concentration and Inequality in the Geographic Distribution of Physicians in the European Union, 2006–2018” (see note 35).
- 39
-
There is no Northern and Western region in the “less developed” category here either.
- 40
-
Ilan Alon et al., “Regime Type and COVID-19 Response”, FIIB Business Review 9, no. 3 (2020): 152–60; Bayerlein et al., “Populism and COVID-19” (see note 9); Gokhan Karabulut et al., “Democracy and COVID-19 Outcomes”, Economics Letters 203, article no. 109840 (2021); David Stasavage, “Democracy, Autocracy, and Emergency Threats: Lessons for COVID-19 from the Last Thousand Years”, International Organization 74, S1 (2020): E1–E17.
- 41
-
Constantin M. Bosancianu et al., “Political and Social Correlates of Covid-19 Mortality”, n. d., https://osf.io/ download/5ee21f239e163700ba8ff580/ (accessed 29 June 2023); Andrés Rodríguez‐Pose and Chiara Burlina, “Institutions and the Uneven Geography of the First Wave of the COVID‐19 Pandemic”, Journal of Regional Science 61, no. 4 (2021): 728–52; Andrea Ascani et al., “The Geography of COVID‐19 and the Structure of Local Economies: The Case of Italy”, Journal of Regional Science 61, no. 2 (2021): 407–41; Marcia C. Castro et al., “Spatiotemporal Pattern of COVID-19 Spread in Brazil”, Science 372, no. 6544 (2021): 821–26.
- 42
-
David Bailey et al., “Regions in COVID-19 Recovery”, Regional Studies 55, no. 12 (2021): 1955–65; Helen Cole et al., “The COVID-19 Pandemic: Power and Privilege, Gentrification, and Urban Environmental Justice in the Global North”, Cities & Health 5, no. S1 (2021): S71–S75.
- 43
-
Armando Cartenì et al., “The Role of Transport Accessibility within the Spread of the CoronaVirus Pandemic in Italy”, Safety science 133, article no. 104999 (2021).
- 44
-
European Commission, “The Regional Impact of COVID-19” (see note 7); Burlina and Rodríguez-Pose, “Inequality, Poverty, Deprivation and the Uneven Spread of COVID-19 in Europe” (see note 23).
- 45
-
Burlina and Rodríguez-Pose, “Inequality, Poverty, Deprivation and the Uneven Spread of COVID-19 in Europe” (see note 23); Richard Blundell et al., “COVID‐19 and Inequalities”, Fiscal Studies 41, no. 2 (2020): 291–319; Tanith C. Rose et al., “Inequalities in COVID19 Mortality Related to Ethnicity and Socioeconomic Deprivation”, MedRxiv, 5 May 2020, doi: 10.1101/2020.04.25.20079491; Faheem Ahmed et al., “Why Inequality Could Spread COVID-19”, The Lancet Public Health 5, no. 5 (2020): e240.
- 46
-
Amaia Calderón-Larrañaga et al., “High Excess Mortality in Areas with Young and Socially Vulnerable Populations during the COVID-19 Outbreak in Stockholm Region, Sweden”, BMJ Global Health 5, no. 10 (2020): e003595; Everton E. Campos de Lima et al., “Spatial Pattern of COVID-19 Deaths and Infections in Small Areas of Brazil”, PLoS One 16, no. 2 (2021): e0246808.
- 47
-
Alessandra Buja et al., “Health and Healthcare Variables Associated with Italy’s Excess Mortality during the First Wave of the COVID-19 Pandemic: An Ecological Study”, Health Policy 126, no. 4 (2022): 294–301; Hugo Pilkington et al., “Spatial Determinants of Excess All-cause Mortality during the First Wave of the Covid-19 Epidemic in France”, BMC Public Health 21, no. 1, article no. 2157 (2021); Ruth Waitzberg et al., “Early Health System Responses to the COVID-19 Pandemic in Mediterranean Countries: A Tale of Successes and Challenges”, Health Policy 126, no. 5 (2022): 465–75.
- 48
-
Marco Travaglio et al., “Links between Air Pollution and COVID-19 in England”, Environmental pollution 268, article no. 115859 (2021); Andrea Pozzer et al., “Regional and Global Contributions of Air Pollution to Risk of Death from COVID-19”, Cardiovascular research 116, no. 14 (2020): 2247–53; Eric S. Coker et al., “The Effects of Air Pollution on COVID-19 Related Mortality in Northern Italy”, Environmental and Resource Economics 76 (2020): 611–34.
- 49
-
Andreas Stang et al., “Excess Mortality Due to COVID-19 in Germany”, Journal of Infection 81, no. 5 (2020): 797–801; Yea-Hung Chen et al., “Excess Mortality in California during the Coronavirus Disease 2019 Pandemic, March to August 2020”, JAMA Internal Medicine 181, no. 5 (2021): 705–07.
- 50
-
Chao Huang et al., “Correlation between Vaccine Coverage and the COVID‐19 Pandemic throughout the World: Based on Real‐world Data”, Journal of Medical Virology 94, no. 5 (2022): 2181–87.
- 51
-
Bishoy L. Zaki et al., “In Trust we Trust: The Impact of Trust in Government on Excess Mortality during the COVID-19 Pandemic”, Public Policy and Administration 37, no. 2 (2022): 226–52.
- 52
-
Constantine Vardavas et al., “Public Perspective on the Governmental Response, Communication and Trust in the Governmental Decisions in mitigating COVID-19 Early in the Pandemic across the G7 Countries”, Preventive Medicine Reports 21, no. 101252 (2021): 1–4.
- 53
-
Jorge Ricardo Ledesma et al., “Evaluation of the Global Health Security Index as a Predictor of COVID-19 Excess Mortality Standardised for Under-reporting and Age Structure”, BMJ Global Health 8, no. 7 e012203 (2023): 1–14.
- 54
-
Ben Ansell et al., “Social Distancing, Politics and Wealth”, West European Politics 44, no. 5–6 (2021): 1283–1313; Anton Gollwitzer et al., “Partisan Differences in Physical Distancing Are Linked to Health Outcomes during the COVID-19 Pandemic”, Nature Human Behaviour 4, no. 11 (2020): 1186–97.
- 55
-
Yea-Hung Chen et al., “Excess Mortality in California by Education during the COVID-19 Pandemic”, American Journal of Preventive Medicine 63, no. 5 (2022): 827–36.
- 56
-
Adekunle Sanyaolu et al., “Comorbidity and Its Impact on Patients with Covid-19”, SN comprehensive clinical medicine 2, no. 8 (2020): 1069–76.
- 57
-
Richard N. van Zyl-Smit et al., “Tobacco Smoking and COVID-19 Infection”, The Lancet Respiratory Medicine 8, no. 7 (2020): 664–65.
- 58
-
Davide Golinelli et al., “Small-scale Spatial Analysis Shows the Specular Distribution of Excess Mortality between the First and Second Wave of the COVID-19 Pandemic in Italy”, Public Health 194 (2021): 182–84.
- 59
-
Sebastien Bourdin et al., “Does Lockdown Work? A Spatial Analysis of the Spread and Concentration of Covid-19 in Italy”, Regional Studies 55, no. 7 (2021): 1182–93; Burlina and Rodríguez-Pose, “Inequality, Poverty, Deprivation and the Uneven Spread of COVID-19 in Europe” (see note 23).
- 60
-
Nicola Ferrara et al., “Relationship between COVID-19 Mortality, Hospital Beds, and Primary Care by Italian Regions: A Lesson for the Future”, Journal of Clinical Medicine 11, no. 14, article no. 4196 (2022); Li-Lin Liang et al., “Covid-19 Mortality Is Negatively Associated with Test Number and Government Effectiveness”, Scientific Reports 10, no. 1 (2020): 1–7.
- 61
-
Committee of the Regions (CoR), “Opinion of the European Committee of the Regions – Equivalent Standards of Living as a Joint Challenge for all Levels of Government in Europe”, Official Journal of the European Union C 440 (18 December 2020): 4–9, https://eur-lex.europa.eu/legal-content/EN/ TXT/PDF/?uri=CELEX:52020IR2612&from=EN (accessed 26 July 2023).
- 62
-
European Commission, “2014–2020 European Structural and Investment Funds”, https://commission.europa. eu/funding-tenders/find-funding/funding-management-mode/ 2014-2020-european-structural-and-investment-funds_en (accessed 26 July 2023).
- 63
-
Eurostat, “Background – The NUTS Classification – An Objective Basis for the Allocation of Funds”, https://ec. europa.eu/eurostat/web/regions/background (accessed 26 July 2023).
- 64
-
“Council Regulation (EC) No 1083/2006 of 11 July 2006 Laying down General Provisions on the European Regional Development Fund, the European Social Fund and the Cohesion Fund and Repealing Regulation (EC) No 1260/1999”, Official Journal of the European Union L 210 (31 July 2006): 25–78, https://eur-lex.europa.eu/legal-content/DE/TXT/PDF/?uri= CELEX%3A32006R1083&%3Bfrom=DE (accessed 26 July 2023).
- 65
-
European Parliament and Council of the European Union, “Regulation (EU) No 1303/2013 of the European Parliament and the Council of 17 December 2013 Laying down Common Provisions on the European Regional Development Fund, the European Social Fund, the Cohesion Fund, the European Agricultural Fund for Rural Development and the European Maritime and Fisheries Fund and Laying down General Provisions on the European Regional Development Fund, the European Social Fund, the Cohesion Fund and the European Maritime and Fisheries Fund and Repealing Council Regulation (EC) No 1083/2006”, Official Journal of the European Union L 347 (20 December 2013): 320–469, https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX: 32013R1303 (accessed 26 July 2023).
- 66
-
Friedrich Heinemann et al., Die Zukunft der EU-Strukturpolitik (Baden-Baden, 2009).
- 67
-
Michael Bayerlein and Matthias Diermeier, Exchanging Money for Love? A Regional Analysis of EU Cohesion Policy on Euroscepticism, Working Paper no. 2219 (Kiel: Kiel Institute for the World Economy, April 2022), https://www.econstor.eu/ bitstream/10419/256926/1/KWP2219.pdf (accessed 26 July 2023).
- 68
-
European Commission, “Kohesio: Discover EU Projects in Your Region”, https://kohesio.acceptance.ec.europa.eu/en/ (accessed 30 June 2023); European Commission, “European Social Fund Plus”, https://ec.europa.eu/european-social-fund-plus/en/projects (accessed 30 June 2023).
- 69
-
Jonathan Watson, Health and Structural Funds in 2007–2013: Country and Regional Assessment, report (Brussels: Directorate-General for Health and Consumer Protection, 9 December 2017), https://hcn.eu/wp-content/uploads/2017/12/9_ WATSON_Health-and-SF-Country-and-regional-assessment. pdf (accessed 26 July 2023).
- 70
-
European Commission, “Kohesio: Improvement of Availability of Quality Health Care Services in Vidzeme Hospital by Developing Health Care Infrastructure”, https://kohesio. acceptance.ec.europa.eu/en/projects/Q3058071 (accessed 30 June 2023).
- 71
-
European Commission, “Kohesio Improving the Availability of Ambulance and Patient Transport Services in Areas with Health Inequalities in Lithuania”, https://kohesio. acceptance.ec.europa.eu/en/projects/Q3780737 (accessed 30 June 2023).
- 72
-
European Commission, “European Social Fund – Projects – Ensuring Sustainable Health Care”, https://ec. europa.eu/esf/main.jsp?catId=46&langId=en&projectId=292 (accessed 30 June 2023).
- 73
-
Sascha O. Becker et al., “Going NUTS: The Effect of EU Structural Funds on Regional Performance”, Journal of Public Economics 94, no. 9–10 (2010): 578–90; Guido Pellegrini et al., “Measuring the Effects of European Regional Policy on Economic Growth: A Regression Discontinuity Approach”, Papers in Regional Science 92, no. 1 (2013): 217–33.
- 74
-
Luisa Gagliardi and Marco Percoco, “The Impact of European Cohesion Policy in Urban and Rural Regions”, Regional Studies 51, no. 6 (2017): 857–68.
- 75
-
Sascha O. Becker et al., “Effects of EU Regional Policy: 1989–2013”, Regional Science and Urban Economics 69 (2018): 143–52.
- 76
-
Giuseppe Albanese et al., Looking for a Star: Evaluating the Effect of the Cohesion Policy on Regional Well-Being, IZA Discussion Paper no. 14521 (Bonn: Institute of Labor Economis [IZA], June 2021), https://papers.ssrn.com/sol3/papers.cfm?abstract_ id=3883797 (accessed 26 July 2023).
- 77
-
Liubove Murauskiene and Marina Karanikolos, “The Role of the European Structural and Investment Funds in Financing Health System in Lithuania: Experience from 2007 to 2013 Funding Period and Implications for the Future”, Health Policy 121, no. 7 (2017): 727–30.
- 78
-
Karina Bedrunka et al., “Identification and Analysis of Structural Fund Support Mitigating the Effects of the COVID-19 Pandemic in the EU – A Case Study of Health Unit Funding”, Energies 14, no. 16, article no. 4976 (2021).
- 79
-
Riccardo Crescenzi et al., “One or Many Cohesion Policies of the European Union? On the Differential Economic Impacts of Cohesion Policy across Member States”, Regional Studies 54, no. 1 (2020): 10–20.
- 80
-
John Bachtler and Colin Wren, “Evaluation of European Union Cohesion Policy: Research Questions and Policy Challenges”, Regional Studies 40, no. 2 (2006) 2, S 143–153; Sarah CE Batterbury, “Principles and Purposes of European Union Cohesion Policy Evaluation”, Regional Studies 40, no. 2 (2006): 179–88; Benedicta Marzinotto, The Growth Effects of EU Cohesion Policy: A Meta-analysis, Bruegel Working Paper no. 2012/14 (Brussels: Bruegel, October 2012), https://www.econstor.eu/ bitstream/10419/78011/1/728570688.pdf (accessed 15 September 2023).
- 81
-
Oana M. Neagu et al., “Addressing Health Inequalities by Using Structural Funds. A Question of Opportunities”, Health Policy 121, no. 3 (2017): 300–06.
- 82
-
Mark McCarthy et al., “Health and the European Structural Funds in the New Member States”, The European Journal of Public Health 23, no. 3 (2013): 522–23.
- 83
-
Katarzyna Dubas-Jakóbczyk and Anna Kozieł, “European Union Structural Funds as the Source of Financing Health Care Infrastructure Investments in Poland – A Longitudinal Analysis”, Frontiers in Public Health 10, article no. 873433 (2022).
- 84
-
Karina Bedrunka et al., “Identification and Analysis of Structural Fund Support Mitigating the Effects of the COVID-19 Pandemic in the EU – A Case Study of Health Unit Funding”, Energies 14, no. 16, article no. 4976 (2021).
- 85
-
Sanjay Budhdeo et al., “Changes in Government Spending on Healthcare and Population Mortality in the European Union, 1995–2010: A Cross-sectional Ecological Study”, Journal of the Royal Society of Medicine 108, no. 12 (2015): 490–98.
- 86
-
Marina Karanikolos et al., “Financial Crisis, Austerity, and Health in Europe”, The Lancet 381, no. 9874 (2013): 1323–31; Bernd Rechel “Funding for Public Health in Europe in Decline?”, Health Policy, 123, no. 1 (2019): 21–26.
- 87
-
McCarthy et al., “Health and the European Structural Funds in the New Member States” (see note 82).
- 88
-
Burlina and Rodríguez-Pose, “Inequality, Poverty, Deprivation and the Uneven Spread of COVID-19 in Europe” (see note 23).
- 89
-
Ivaldi et al., “Objective and Subjective Health” (see note 35).
- 90
-
Theo Hitiris and John Posnett, “The Determinants and Effects of Health Expenditure in Developed Countries”, Journal of Health Economics 11, no. 2 (1992): 173–81.
- 91
-
Sofia Xesfingi and Athanassios Vozikis, “Patient Satisfaction with the Healthcare System: Assessing the Impact of Socio-economic and Healthcare Provision Factors”, BMC Health Services Research 16, no. 1 (2016): 1–7.
- 92
-
European Commission, “EU4Health Programme 2021–2027 – A Vision for a Healthier European Union”, https:// health.ec.europa.eu/funding/eu4health-programme-2021-2027-vision-healthier-european-union_en (accessed 4 July 2023).
- 93
-
Greer et al., Everything You Always Wanted to Know about European Union Health Policy (see note 2).
- 94
-
German Federal Ministry of Health (BMG), “EU4Health – Aktionsprogramm der Europäischen Union im Bereich der Gesundheit”, https://www.bundesgesundheitsministerium. de/themen/internationale-gesundheitspolitik/europa/ eu4health.html (accessed 26 July 2023).
- 95
-
European Commission, “Questions and Answers on the New EU4Health Programme”, https://ec.europa.eu/ commission/presscorner/detail/en/qanda_20_956 (accessed 4 July 2023).
- 96
-
European Commission, “Horizon Europe”, https:// research-and-innovation.ec.europa.eu/funding/funding-opportunities/funding-programmes-and-open-calls/horizon-europe_en (accessed 4 July 2023).
- 97
-
European Union, “What Is the InvestEU Programme?”, https://investeu.europa.eu/what-investeu-programme_en (accessed 4 July 2023).
- 98
-
European Commission, “Find investment opportunities”, https://ec.europa.eu/investeuportal/desktop/en/card-view.html (accessed 4 July 2023).
- 99
-
European Commission, “The Recovery and Resilience Facility”, https://commission.europa.eu/business-economy-euro/economic-recovery/recovery-and-resilience-facility_en (accessed 4 July 2023).
- 100
-
European Commission, “Project – Enhancing Primary Health Care”, https://commission.europa.eu/projects/ enhancing-primary-health-care_en (accessed 4 July 2023).
- 101
-
European Commission, “Project – Czech Oncology Institute”, https://commission.europa.eu/projects/czech-oncology-institute_en (accessed 4 July 2023).
- 102
-
In the period under study, no regions in Northern and Western EU member states qualified for cohesion funding.
- 103
-
In the period under study, no regions in Northern and Western EU member states qualified for cohesion funding.
- 104
-
Becker et al., “Going NUTS: The Effect of EU Structural Funds on Regional Performance” (see note 73).
- 105
-
Paolo Di Caro et al., “One Policy, Different Effects: Estimating the Region‐specific Impacts of EU Cohesion Policy”, Journal of Regional Science 62, no. 1 (2022): 307–30.
- 106
-
Becker et al., “Effects of EU Regional Policy: 1989–2013” (see note 75).
- 107
-
Vanessa A. Boese-Schlosser et al., Trust Issues? How Being Socialised in an Autocracy Shapes Vaccine Uptake, WZB Discussion Paper SP V 2023-502 (Berlin: Wissenschaftszentrum Berlin für Sozialforschung, November 2023).
- 108
-
Antoni Rangachev et al., “The Demographic and Geographic Impact of the COVID Pandemic in Bulgaria and Eastern Europe in 2020”, Scientific Reports 12, no. 1, article no. 6333 (2022); Gergő Túri et al., “Riding the Pandemic Waves – Lessons to Be Learned from the COVID-19 Crisis Management in Romania”, Tropical Medicine and Infectious Disease 7, no. 7, article no. 122 (2022).
- 109
-
Antoni Rangachev et al., “The Impact and Progression of the COVID-19 Pandemic in Bulgaria in Its First Two Years”, Vaccines 10, no. 11, article no. 1901 (2022); Stefan Dascalu et al., “COVID-19 in Romania: What Went Wrong?” Frontiers in Public Health 9, article no. 813941 (2021).
- 110
-
Bayerlein et al., “Populism and COVID-19” (see note 9).
- 111
-
Michael Bayerlein, “Die Europäische Gesundheitsunion”, in Stand der Integration, ed. Raphael Bossong and Nicolai von Ondarza (Berlin: Stiftung Wissenschaft und Politik, forthcoming 2024).
- 112
-
Greer et al., Everything You Always Wanted to Know about European Union Health Policy (see note 2).
- 113
-
Will Jennings et al., “Trust and Vaccine Hesitancy during the COVID-19 Pandemic: A Cross-national Analysis”, Vaccine: X 14, no. 100299 (2023): S. 1–9; Olivier Bargain and Aminjonov Ulugbek, “Trust and Compliance to Public Health Policies in Times of COVID-19”, Journal of Public Economics 192, no. 104316 (2020): 1–13.
- 114
-
European Commission, “The Regional Impact of COVID-19” (see note 7).
All rights reserved.
© Stiftung Wissenschaft und Politik, 2024
SWP Research Papers are peer reviewed by senior researchers and the executive board of the Institute. They are also subject to copy-editing. For further information on our quality control procedures, please visit the SWP website: https://www.swp-berlin.org/ en/about-swp/quality-management-for-swp-publications/.
SWP Research Papers reflect the views of the author(s).
SWP
Stiftung Wissenschaft und Politik
German Institute for International and Security Affairs
Ludwigkirchplatz 3–4
10719 Berlin
Germany
Phone +49 30 880 07-0
Fax +49 30 880 07-200
www.swp-berlin.org
swp@swp-berlin.org
ISSN (Print) 2747-5123
ISSN (Online) 1863-1053
DOI: 10.18449/2024RP01
Translation by Tom Genrich
(English version of SWP‑Studie 15/2023)